Norplant as a contraceptive device in enugu, eastern nigeria
Advances in Contraception, 1998; 14: 109^119.
# 1998 Kluwer Academic Publishers. Printed in the Netherlands
Norplant* as a contraceptive device in Enugu,
B. OZUMBA (1), W. CHUKUDEBELU (1) and R. SNOW (2)
(1) Department of Obstetrics and Gynecology, University of Nigeria Teaching Hospital,
(2)Department of Population Sciences, Harvard School of Public Health, Boston,
This paper is an evaluation of acceptability and use-experience with the
contraceptive device Norplant at the University of Nigeria Teaching Hospital,
Enugu, Eastern Nigeria. Over a period of 36 months, 173 women (8% of the
clinic population) accepted the implant. Use of Norplant was concentrated
among high-parity women, and the proportion of Norplant users was highest
among women aged 30^34 years. Comparing Norplant and IUD users, we
found Norplant users to be signi¢cantly less highly educated with 51% of
Norplant users having tertiary education compared to 25% of new IUD users.
The continuation rate with Norplant was 89% at three years, suggesting this
method has the potential for improving the low contraceptive prevalence in this
Contraceptive use in sub-Saharan Africa is low by international standards [1], and
Nigeria has one of the lowest contraceptive prevalence rates in Africa, currently at
6% [2]. The Nigeria Fertility Survey [3] reports that only 46% of Nigerian women
know of a family planning method. The health hazards associated with high parity
are well known. Maternal morbidity and mortality are very high in Nigeria [4] and
the reproductive health of women can only be enhanced if they are provided with an
opportunity to plan their reproductive lives. Safe provision of various contraceptive
*Norplant is the registered trademark of the Population Council for subdermal
methods to the general population is crucial to the enhancement of women's
reproductive and general health. Norplant as a family planning device is relatively
new in Nigeria, having been introduced into clinical practice at the University of
Nigeria Teaching Hospital (UNTH) Enugu in 1992. The family planning clinic of the
hospital has been in operation since 1973, o¡ering the IUD, depot norethisterone
enanthate, oral contraception, vaginal foam, condom and tubal ligation. We
evaluated the acceptability of Norplant in this community to assess its potential
value to couples in the region and country at large.
The UNTH is located in Enugu, the political and population center of the Igbos of
Eastern Nigeria. In consonance with its recently promulgated national population
policy [5], the federal government of Nigeria, in 1993, designated UNTH as the
headquarters for the eastern zone of its tertiary reproductive health center project.
The program's functions are aimed at population activities including fertility,
sexually transmitted diseases (STDs), and acquired immunode¢ciency syndrome
(AIDS) control, as well as maternal health. The activities of this center cover all of
Eastern Nigeria with a population of about 20 million people. The responsibilities of
the tertiary center include the training of personnel and supervision of services in the
general hospitals and primary health centers within the zone. UNTH is well suited
for evaluation of Norplant's likely acceptability in the region and for appropriate
dissemination of information and skill regarding Norplant.
The aim of this study was to describe women who are using Norplant as a family
planning measure in Enugu, Eastern Nigeria, and to examine how these women
di¡er from women using the IUD. A 3-year retrospective cross-sectional review of
Norplant users was carried out from June 1992 to May 1995 and compared the
Norplant users with women using the IUD for family planning during the same
period. The IUD was chosen for comparison because it is provider-dependent, as is
Norplant, and is the method used by the largest segment of family planning
attendees. It is a well-known method and, therefore, does not elicit fears often
At the family planning clinics, groups of patients were given a well-balanced
presentation of the di¡erent methods of contraception by nurses. Those who
accepted were then seen by doctors and questioned about age, parity, educational
status, ¢rst informants on Norplant, and primary reason for using the implant.
Individual client counselling was provided by doctors and Norplant acceptors were
informed about the bene¢ts and side-e¡ects of the implant. The acceptors were given
an opportunity to ask questions and were told to report to the clinic immediately if
they observed any problems including infection, migration of the implant, menstrual
irregularity or pregnancy. They were also told to report for removal of the implant
immediately after the ¢ve-year duration had expired. Informed consent was obtained
from Norplant acceptors and they were physically examined to rule out medical
contraindications before insertion. Norplant, consisting of sets of six levonorgestrel-
Norplant as a Contraceptive Device in Enugu, Eastern Nigeria
releasing silastic capsules, was inserted by doctors in the upper arm. Follow-up visits
were arranged at 1-, 3- and 6-monthly intervals for the ¢rst 12 months, and
subsequently every 12 months unless there were complications. A total of 173 women
accepted Norplant during the 3-year period, while 1298 women chose the IUD.
Sociodemographic characteristics of Norplant and IUD acceptors were compared,
as well as their sources of information about Norplant and their primary reason for
choosing it. Based on a total of 4266 woman-months of use accumulated over three
years, complications and discontinuation rates were also obtained and subsequently
Training of physicians and nurses to provide Norplant was conducted annually at a
national level and at 6-monthly intervals at the regional centers. Twelve consultant
gynecologists and 20 resident gynecologists at the teaching hospital were trained in
the proper technique of insertion and removal of the implant. Physicians in
peripheral centers who are interested in family planning are encouraged to attend
the training sessions conducted at the center. Each training session lasts 2 weeks and
accommodates ¢ve physicians and ¢ve nurses. E¡orts are made to provide enough
removal cases to serve the training needs. Doctors and nurses are trained in proper
counselling techniques which will help the clients make an informed choice of
Physicians and nurses who have been trained to provide Norplant both within and
outside the teaching hospital commend its use. This will help to expand the use of the
implant outside Enugu. The major constraint to its use in Enugu and its environment
is the very limited supply from the donor agencies.
All data were analyzed using SAS statistical software version 6.1 (SAS Institute Inc.,
Cary, NC) [6]. The statistical evaluation of categorical data was based on Pearson's w2
test. Continuous and ordinal data were evaluated using t-tests and W|lcoxon's rank
sum statistic, respectively. Results were presented as the mean(+SD); p-levels of
Types of contraceptive methods accepted at the clinic and percentage distribution
Table 1 shows the types of contraceptive methods accepted by all clients visiting the
family planning clinic at UNTH from June 1992 to May 1995. The IUD was
accepted by the largest percentage of women (63%), with the oral contraceptive pill
and sterilization by tubal ligation being the least acceptable (1% each). Norplant was
the method of choice for 8% of the women.
Table 1. Distribution of contraceptive methods accepted by clients at UNTH from June 1992 to
*Two-monthly injection of norethisterone enanthate
Age distribution of Norplant and IUD acceptors
The age ranges of both the Norplant and IUD acceptors were symmetrical in
distribution (Figure 1). The mean age of Norplant acceptors was 33.9+5.0 and that
of IUD users 32.5+5.9 years (p50.5). Most notably, acceptors of IUDs were more
likely to be 535 years (62% were 535 years, 38%535 years) while acceptors of
Norplant represented a more balanced distribution of the reproductive age of women
(51% were 535 years, 49% 535 years, p50.05). There were no Norplant users below
Figure 1. Comparison of age distribution in years of Norplant and IUD acceptors. Norplant
Norplant as a Contraceptive Device in Enugu, Eastern Nigeria
Parity distribution of Norplant and IUD acceptors
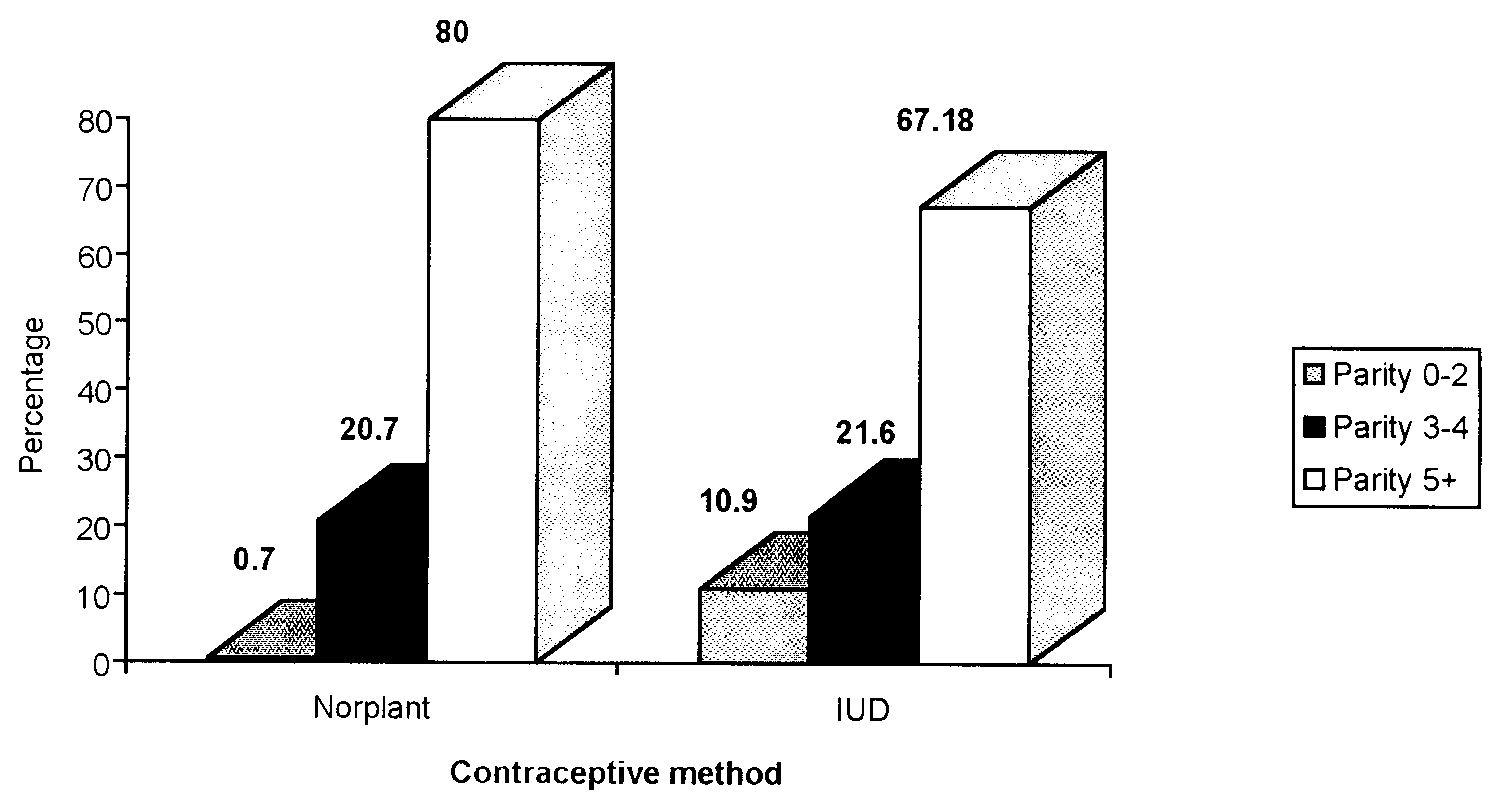
The parity distributions of Norplant and IUD acceptors is shown graphically in
Figure 2. The mean parity of Norplant acceptors was 6.4+1.9 and that of IUD
acceptors was 5.5+2.8 (p50.05). Eighty percent of Norplant acceptors had 5 or
more children, while only 67% of IUD users were parity 5 and above. Parity 0^2
comprised only 0.7% of Norplant acceptors but 11% of IUD users. All Norplant
acceptors had delivered one or more babies whereas 3 IUD users were nulliparous.
Figure 2. A comparison of parity distribution between Norplant and IUD acceptors. Norplant
Figure 3 illustrates the disparity in educational status among Norplant and IUD
acceptors. Less than 1% of Norplant acceptors had tertiary education while 25% of
IUD users were from this high educational group. Twenty-four percent of Norplant
acceptors had no formal education, a similar proportion being found among IUD
acceptors. Likewise 41% of Norplant acceptors and 40% of IUD acceptors had
attended elementary school. There was a disparity among the proportion of Norplant
and IUD acceptors with secondary education: 34% of Norplant acceptors had
secondary education compared to 11% of IUD acceptors. When controlling for age,
there remained a signi¢cant di¡erence in educational attainment between Norplant
and IUD users with Norplant users having lower educational attainment. The
di¡erence in educational status between Norplant and IUD users was sustained
Figure 3. Comparison of educational status between Norplant and IUD acceptors. Norplant
Additional features of Norplant acceptors
Source of initial information about Norplant among acceptors
One hundred and forty-three Norplant acceptors responded to the question about
where they ¢rst heard of Norplant. Table 2 indicates that nurses were the most
signi¢cant source of initial information about the method (61%). The mass media
(comprising print and electronic media) provided information for 12%, spouses for
Eighty-three Norplant acceptors responded to the question about what was the
primary reason for choosing Norplant to limit their family size. The principal reasons
for accepting Norplant as a contraceptive measure are listed in Table 3. Seventy
percent of respondents felt that they had achieved the desired family size. Economic
considerations were cited by another 21%, while declining health was given as a
Norplant as a Contraceptive Device in Enugu, Eastern Nigeria
Table 2. Source of initial information about Norplant among acceptors at UNTH from June
Table 3. Primary reason for limiting family size among Norplant acceptors at UNTH from June
Table 4. Reasons for removal of Norplant among 173 acceptors at UNTH from June 1992 to
Table 4 shows why Norplant had to be discontinued by 12 of the 173 acceptors.
Abnormality of menstruation was responsible for the highest number of removals (10
of 12). Amenorrhea, dermatitis at site of insertion and raised blood pressure were
each responsible for one removal. Menorrhagia was the most common complaint [6],
followed by irregular menses [3]. The continuation rates of Norplant use among the
women were 99.4% at 3 months, 98.1% at 6 months, 94.5% at 12 months, 92.5% at 24
This study shows that Norplant acceptors in Enugu, Eastern Nigeria tended to be
older, of higher parity, and less highly educated than IUD acceptors from the same
community. The IUD acceptors were mostly less than 35 years of age while Norplant
acceptors demonstrated a more even spread across the reproductive age of women.
The age distribution of Norplant acceptors di¡ers among di¡erent studies. The mean
age ranges from 24.8 years in Brasil to 32.5 years in Egypt [7,8]. Consistent with our
¢ndings, the mean age of IUD users was lower than that of Norplant users in the
Brasilian and Egyptian studies, 24.5 and 31.9 years, respectively.
Few women accepted Norplant before delivery of three of more children, while 10%
of IUD acceptors had 0^2 children. Norplant acceptors were likely to be high-parity
women, with 80% being parity 5 and above. The signi¢cant di¡erence in the mean
parities of the Norplant and IUD users reinforces our ¢nding that use of Norplant was
principally to limit family size. Similar to our data, the majority of the women (93%) in
the study from Egypt chose Norplant when they had attained their desired family size
[7]. In the report from San Francisco, USA [9], as many as 38% of Norplant acceptors
chose the device to limit their family size [10]. The mean parity of Norplant acceptors
varies from 2.3 in the Dominican Republic where it is mostly used for birth spacing to
5.9 in Egypt where it was chosen mainly to limit family size [8,9]. In our study the mean
parity was 6.4 and association between high parity and Norplant acceptors is
consistent with the reason for choosing the implant. Educational status of the women
was an important factor determining their acceptance of Norplant. Women with the
highest education were not represented among new Norplant acceptors in contrast to
IUD acceptors. Women with tertiary education may be more likely to have access to
information on Norplant from the international media. Some of the reservations
expressed about the implant by the media [10] such as the possibility of migration may
make women initially wary of embracing its use. In a report from San Francisco, USA
[10], 10% of Norplant acceptors had a college degree.
Educational status is known to in£uence reproductive behavior [11]. Educated
women are more likely to use contraceptives in Nigeria [12] and in this case women
with secondary education were more willing to accept Norplant than the IUD.
Ruminjo et al. [13] reported that Norplant acceptors in Nairobi, Kenya had achieved
a higher educational status than acceptors of female voluntary surgical contraception
Norplant as a Contraceptive Device in Enugu, Eastern Nigeria
by minilaparotomy (secondary or university education, 64% vs. 36.5%). Possibly the
women with higher education were more willing to try more modern methods of
Most Norplant acceptors traced their source of information regarding the device
to nurses, probably because at the UNTH family planning clinic, nurses hold
counselling sessions every morning for family planning attendees. The mass media
also played an important role in promoting awareness of Norplant in the community,
being the second greatest source of information on the device. In a study in San
Francisco, USA [10], the media played a similar role and was the second main source
of information on the device after the family planning clinic. Doctors provided
information that led to acceptance of Norplant in only 8% of cases. Clinicians and
government o¤cials in some developing countries, such as Indonesia and Thailand,
have occasionally been charged with coercing women to accept and keep the implant
[14,15]. This does not appear to be the case in Eastern Nigeria. This healthy
beginning augurs well for its introduction to a larger segment of the Nigerian
The continuation rate of 95% at one year noted in this study is comparable to 95%
in Chile and 94% in China [16]. A lower level (80%) in Scandinavia and a high of 99%
in Sri Lanka have also been reported [16]. The continuation rate of a contraceptive
device varies from country to country and depends upon individual acceptor
characteristics such as age, parity and education [17,18]. For a device such as
Norplant requiring clinical cooperation for removal, the accessibility and quality of
service can have an important impact on the continuation rate. For this reason, at the
UNTH, training of doctors in the proper technique for insertion and removal of
Norplant is emphasized and patients are advised to report to the clinic if they have
any complications. Menstrual irregularity led to most of the discontinuations in this
study, and has been reported to be the most frequent and signi¢cant complaint in
other settings [19]. Reports from other studies [20,21] have cited medical conditions
including headache, excessive weight gain and cardiovascular problems as signi¢cant
complaints leading to discontinuation of the implants. This was not the case in this
study, as only one woman ceased to use Norplant because she developed hyperten-
sion while on the implant. The absence of these medical conditions as reasons for
discontinuation may result from adequate selection of cases and counselling received
by the clients. Nigeria's total fertility rate of 6 [2] is one of the highest in Africa, and
the fertility rate of the locality studied may be higher than the overall national rate.
Tradition, in some parts of Eastern Nigeria, honors women who deliver 9 or more
children in their lifetime. At the occasion of the 9th birth, a goat is slaughtered to
celebrate what is called the `ewu ukwu' [22] ceremony (roughly translated as `goat for
pelvis'). Strong belief in reincarnation in the local community includes a common
fear that sterilization will lead to sterility when a woman or man returns in the `next
life'. Thus Norplant, which is long-acting and reversible, may have a special appeal
among women who want to limit family size, but who fear `after life' consequences of
sterilization. The choice of Norplant by many women as an alternative to steriliza-
tion has also been reported from the UK [23]. Long-acting methods such as Norplant
may, therefore, be ful¢lling an unmet need for contraception in this community.
Results from this study show that Norplant is safe and acceptable to a small sector
of Nigerian women, characterized by high parity, older age, and moderate (but not
high) educational status. Norplant appears to have made an impact among family
planning clients at the university teaching hospital because within 3 years of its
inception, 8% of the women had accepted it as their family planning method. The
acceptance rate has remained constant within this period. It is possible that
introduction of Norplant into our family planning practice will attract high-parity
women who are averse to sterilization. Sexually transmitted diseases are thought to
be highly prevalent in Nigeria and Africa, as are many other communicable diseases
[24]. This may make Norplant a more appropriate contraceptive method than the
IUD for clients with a high risk of acquiring sexually transmitted diseases such as
teenagers and sex workers. The introduction of a safe and acceptable family planning
method will go a long way to increase the currently low contraceptive prevalence in
the country. This will consequently improve the general health and socioeconomic
This paper was written during Dr B.C. Ozumba's 1-year leave at the Harvard School
of Public Health as a Takemi Fellow in International Health with funds provided by
We are grateful to Professor Michael Reich for his assistance and comments
during the preparation of the text. We also thank Dr Grace Wyshack for her help
1. Alihonou E, Carre N, Capochiohi V, Thonneau P. Contraceptive continuation and its determinants in
Benin. Contraception. 1997;55:97^102.
2. Federal O¤ce of Statistics. Nigeria Demographic and Health Survey, 1990. Columbia, 1992, MD.
3. Nigeria Fertility Survey [1981^1982]. In: World Fertility Survey, Prinicipal Report: Methodology and
Findings, Vol. 1. Voorburg, Netherlands 1982, International Statistical Institute.
4. Chukudebelu WO, Ozumba BC. Maternal mortality at the University of Nigeria Teaching Hospital,
Enugu: a 10 year survey. Trop J Obstet Gynecol. 1980;1:23^4.
5. Federal Republic of Nigeria. National Policy on Population for Development Unity, Progress and Self-
6. SAS Institute Inc. SAS/STAT User's Guide, Vols 1 and 2, Version 6.11, 4th edn. Cary, NC, SAS
7. Hardy E, Goodson P. Association between contraceptive method accepted and perception of
information received: a comparison of Norplant and IUD acceptors. Contraception. 1990;43:121^8.
8. Shaaban MM, Salah M. A two year experience with Norplant implants in Assiut, Egypt, 1984.
9. Alvarez F, Brache V, Faunders A. The clinical performance of Norplant implants over time. A
comparison of two cohorts. Stud Fam Plann. 1988;19:118^24.
10. Darney PD et al. Acceptance and perceptions of Norplant among users in San Francisco, USA. Stud
Norplant as a Contraceptive Device in Enugu, Eastern Nigeria
11. Jain A, Nag M. Importance of female primary education for fertility reduction in India 1986. Econ
12. Oni G, McCarthy J. Use of contraceptives for birth spacing in a Nigerian City, 1986. Stud Fam Plann.
13. Rumnijo JK, Achwal I, Ruminjo IN. A comparative study of users of long-term contraceptive subdermal
implants and female surgical contraception in Kenya, 1994. East Afr Med J. 1988;70:552^63.
14. Ward JS, Poernomo Sigit Sidi I, Simmons R, Simmons GB. Service delivery systems and quality of care
in the implementation of Norplant in Indonesia. New York, The Population Council. Unpublished
15. Zimmerman M et al. Assessing the acceptability of Norplant implants in four countries. Findings from
Focus Group Research. Stud Fam Plann. 1990;21:92^103.
16. Sivin I. International experience with Norplant and Norplant 2 contraceptives. Stud Fam Plann.
17. Kreager P. Family Planning Drop-Outs Reconsidered: A Critical Review of Research and Research
Findings. Research for Action No. 3, 1986. London, International Planned Parenthood Federation.
18. Mauldin W, Parker M. Experience with Contraceptive Methods in Less Developed Countries. Centre
for Policy Studies Working Paper, No. 30. New York, The Population Council; 1978.
19. Diaz S et al. Clinical assessment of treatments for prolonged bleeding in users of Norplant implants,
1990. Contraception. 1990;42:97^107.
20. Du MK, Zheng HM, Chen HC, Chow LP. Study of Norplant implants in Shanghai: three year
experience. Int J Obstet Gynecol. 1990;33:345^52.
21. Basnayake S, Thapa S, Balogh SA. Evaluation of safety, e¤cacy and acceptability of Norplant implants
in Sri Lanka. Stud Fam Plann. 1988;19:39^52.
22. Egwuatu VE. Childbearing among the Igbos of Nigeria. Int J Obstet Gynecol. 1986;24:103^11.
23. Davie J, Hirematu K, Glasier A. The introduction of a new contraceptive: two years experience with
Norplant. Health Bull Edin. 1996;54:314^22.
24. Osoba AO. Sexually transmitted diseases in Nigeria: a review of the present situation. W Afr J Med.
Le pre¨sent expose¨ consiste en une e¨valuation e¡ectue¨e a l'hoªpital universitaire d'Enugu au Nige¨ria
occidental en ce qui concerne l'acceptabilite¨ et l'expe¨rience en matiere d'utilisation du dispositif contra-
ceptif Norplant. Au cours d'une pe¨riode de trente six mois, cent soixante treize femmes (repre¨sentant huit
pour cent de la population de la clinique) ont accepte¨ de porter les implants. L'utilisation de Norplant
pre¨dominait chez des meres de familles nombreuses et la proportion d'utilisatrices de Norplant e¨tait la plus
e¨leve¨e chez les femmes de 30 a 34 ans. La comparaison entre utilisatrices de Norplant et de DIU a fait
ressortir que les premieres e¨taient beaucoup moins instruites: moins d'un pour cent des utilisatrices de
Norplant avaient rec°u une e¨ducation du niveau tertiaire, compare¨es a 25 pour cent pour les utilisatrices de
DIU. Le taux de poursuite du port des implants e¨taient de 89% au terme de trois ans, donnant a penser que
cette me¨thode est susceptible d'ame¨liorer le faible recours a la contraception dans cette re¨gion.
Este trabajo es una evaluacio¨n de la aceptabilidad y la experiencia en el uso del dispositivo anticonceptivo
Norplant en el Hospital Escuela de la Universidad de Nigeria, Enugu, regio¨n oriental de Nigeria. Durante
un per|¨odo de treinta y seis meses, ciento setenta y tres mujeres (que representaban el 8% de la poblacio¨n
cl|¨nica) aceptaron el implante. El uso de Norplant se concentro¨ entre las mujeres de alta paridez y las
proporciones de usuarias de Norplant sen¬alaron el nivel ma¨ximo entre mujeres de 30 a 34 an¬os de edad. Al
compararse las aceptadoras de Norplant y de DIU, se determino¨ que las usuarias de Norplant ten|¨an un
nivel de educacio¨n signi¢cativamente menor: menos del 1% de las aceptadoras de Norplant hab|¨a
concluido la educacio¨n terciaria, en comparacio¨n con el 25% de las nuevas usuarias de DIU. La tasa de
continuacio¨n con Norplant era del 89% al cabo de tres a·os, lo cual sugiere que este me¨todo tiene el
potencial de mejorar la baja frecuencia de anticonceptivos en esta regio¨n.
Articles Medical therapy to facilitate urinary stone passage: a meta-analysis John M Hollingsworth, Mary A M Rogers, Samuel R Kaufman, Timothy J Bradford, Sanjay Saint, John T Wei, Brent K Hollenbeck Summary Background Medical therapies to ease urinary-stone passage have been reported, but are not generally used. If eff ective, Lancet 2006; 368: 1171–79 such therapies would incr
REGULAMENTO PROMOÇÃO ESCOLA DO ROCK A empresa Coopershoes – Coop. Calçados e Comp. Joanetense Ltda., inscrita no CNPJ/MF sob o nº 02.675.611/0001-65, com endereço na Rua Vicente Prieto, n.º 3581, Joaneta, Picada Café, Rio Grande do Sul , detentora da marca CONVERSE, doravante denominada simplesmente CONVERSE, nos termos da Lei nº 5.768/1971, regulamentada pelo Decreto nº 70.951/1972, pr
 Advances in Contraception, 1998; 14: 109^119.
Advances in Contraception, 1998; 14: 109^119.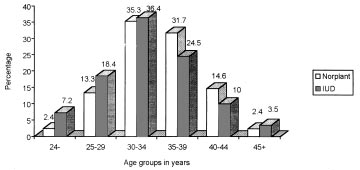 Table 1. Distribution of contraceptive methods accepted by clients at UNTH from June 1992 to
*Two-monthly injection of norethisterone enanthate
Age distribution of Norplant and IUD acceptors
The age ranges of both the Norplant and IUD acceptors were symmetrical in
distribution (Figure 1). The mean age of Norplant acceptors was 33.9+5.0 and that
of IUD users 32.5+5.9 years (p50.5). Most notably, acceptors of IUDs were more
likely to be 535 years (62% were 535 years, 38%535 years) while acceptors of
Norplant represented a more balanced distribution of the reproductive age of women
(51% were 535 years, 49% 535 years, p50.05). There were no Norplant users below
Figure 1. Comparison of age distribution in years of Norplant and IUD acceptors. Norplant
Table 1. Distribution of contraceptive methods accepted by clients at UNTH from June 1992 to
*Two-monthly injection of norethisterone enanthate
Age distribution of Norplant and IUD acceptors
The age ranges of both the Norplant and IUD acceptors were symmetrical in
distribution (Figure 1). The mean age of Norplant acceptors was 33.9+5.0 and that
of IUD users 32.5+5.9 years (p50.5). Most notably, acceptors of IUDs were more
likely to be 535 years (62% were 535 years, 38%535 years) while acceptors of
Norplant represented a more balanced distribution of the reproductive age of women
(51% were 535 years, 49% 535 years, p50.05). There were no Norplant users below
Figure 1. Comparison of age distribution in years of Norplant and IUD acceptors. Norplant
 Norplant as a Contraceptive Device in Enugu, Eastern Nigeria
Parity distribution of Norplant and IUD acceptors
The parity distributions of Norplant and IUD acceptors is shown graphically in
Figure 2. The mean parity of Norplant acceptors was 6.4+1.9 and that of IUD
acceptors was 5.5+2.8 (p50.05). Eighty percent of Norplant acceptors had 5 or
more children, while only 67% of IUD users were parity 5 and above. Parity 0^2
comprised only 0.7% of Norplant acceptors but 11% of IUD users. All Norplant
acceptors had delivered one or more babies whereas 3 IUD users were nulliparous.
Norplant as a Contraceptive Device in Enugu, Eastern Nigeria
Parity distribution of Norplant and IUD acceptors
The parity distributions of Norplant and IUD acceptors is shown graphically in
Figure 2. The mean parity of Norplant acceptors was 6.4+1.9 and that of IUD
acceptors was 5.5+2.8 (p50.05). Eighty percent of Norplant acceptors had 5 or
more children, while only 67% of IUD users were parity 5 and above. Parity 0^2
comprised only 0.7% of Norplant acceptors but 11% of IUD users. All Norplant
acceptors had delivered one or more babies whereas 3 IUD users were nulliparous.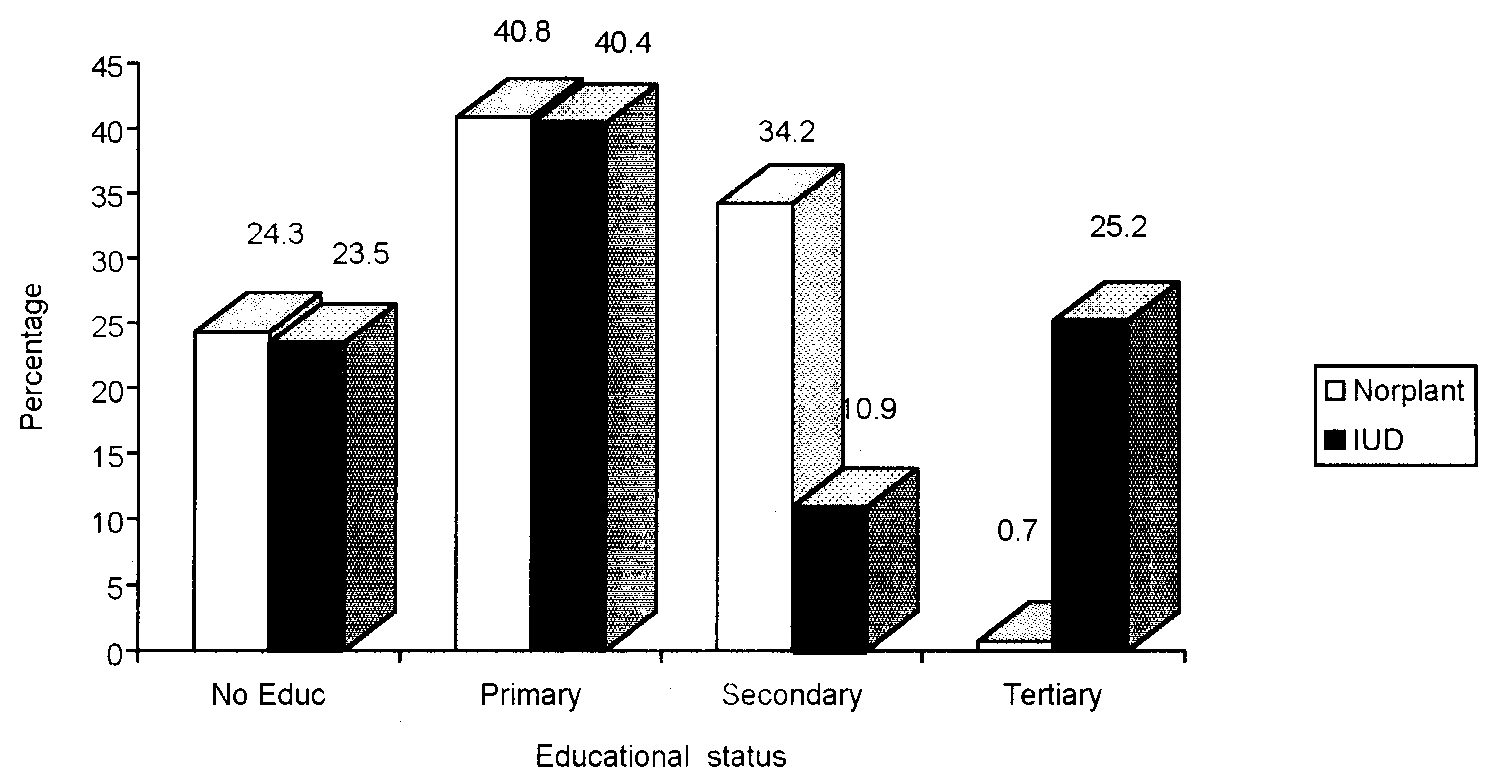 Figure 3. Comparison of educational status between Norplant and IUD acceptors. Norplant
Additional features of Norplant acceptors
Source of initial information about Norplant among acceptors
One hundred and forty-three Norplant acceptors responded to the question about
where they ¢rst heard of Norplant. Table 2 indicates that nurses were the most
signi¢cant source of initial information about the method (61%). The mass media
(comprising print and electronic media) provided information for 12%, spouses for
Eighty-three Norplant acceptors responded to the question about what was the
primary reason for choosing Norplant to limit their family size. The principal reasons
for accepting Norplant as a contraceptive measure are listed in Table 3. Seventy
percent of respondents felt that they had achieved the desired family size. Economic
considerations were cited by another 21%, while declining health was given as a
Norplant as a Contraceptive Device in Enugu, Eastern Nigeria
Table 2. Source of initial information about Norplant among acceptors at UNTH from June
Table 3. Primary reason for limiting family size among Norplant acceptors at UNTH from June
Table 4. Reasons for removal of Norplant among 173 acceptors at UNTH from June 1992 to
Table 4 shows why Norplant had to be discontinued by 12 of the 173 acceptors.
Figure 3. Comparison of educational status between Norplant and IUD acceptors. Norplant
Additional features of Norplant acceptors
Source of initial information about Norplant among acceptors
One hundred and forty-three Norplant acceptors responded to the question about
where they ¢rst heard of Norplant. Table 2 indicates that nurses were the most
signi¢cant source of initial information about the method (61%). The mass media
(comprising print and electronic media) provided information for 12%, spouses for
Eighty-three Norplant acceptors responded to the question about what was the
primary reason for choosing Norplant to limit their family size. The principal reasons
for accepting Norplant as a contraceptive measure are listed in Table 3. Seventy
percent of respondents felt that they had achieved the desired family size. Economic
considerations were cited by another 21%, while declining health was given as a
Norplant as a Contraceptive Device in Enugu, Eastern Nigeria
Table 2. Source of initial information about Norplant among acceptors at UNTH from June
Table 3. Primary reason for limiting family size among Norplant acceptors at UNTH from June
Table 4. Reasons for removal of Norplant among 173 acceptors at UNTH from June 1992 to
Table 4 shows why Norplant had to be discontinued by 12 of the 173 acceptors.