patients in each study group may have been relatively
4. Kostis JB. Pharmacological differentiation of angiotensin-converting enzyme
low, which may have compromised statistical power in
inhibitors. J Human Hyperten 1989;3:119 –125. 5. Brown NJ, Vaughan DE. Angiotensin-converting enzyme inhibitors. Circula-
detecting a clinically meaningful difference. However,
given the results of our study, we estimate Ն80% power
6. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in
to detect a clinically meaningful relative risk reduction of
high-risk patients. The Heart Outcomes Prevention Evaluation Study Investiga-
30% in the primary outcome among groups. Our study is
tors. N Engl J Med 2000;342:145–153.
the first direct comparison of ACE inhibitors in terms of
7. Tu K, Mamdani MM, Jacka RM, Forde NJ, Rothwell DM, Tu JV. The striking effect of the Heart Outcomes Prevention Evaluation (HOPE) on ramipril pre-
heart failure effectiveness. Our results suggest no signif-
scribing in Ontario. Can Med Assoc J 2003;168:553–557.
icant differences among patient ACE inhibitors in clini-
8. Furberg CD, Pitt B. Are all angiotensin-converting enzyme inhibitors inter-
cally meaningful outcomes for treating patients with
changeable? J Am Coll Cardiol 2001;37:1456 –1460. 9. Sica DA. Class effects of angiotensin-converting enzyme inhibitors. Am J
CHF. Thus, when prescribing ACE inhibitors, con-
Manag Care 2000;6:S85–S108.
sideration should likely be given to dosing conve-
10. Jong P, Gong Y, Liu PP, Austin PC, Lee DS, Tu JV. Care and outcomes of patients newly hospitalized for heart failure in the community treated by cardi-
ologists compared with other specialists. Circulation 2003;108:184 –191. 11. Glesby MJ, Hoover DR. Survivor treatment selection bias in observational studies: examples from the AIDS literature. Ann Intern Med 1996;124:999 –1005. 12. Schneeweiss S, Seeger JD, Maclure M, Wang PS, Avorn J, Glynn RJ. 1. Garg R, Yusuf S. Overview of randomized trials of angiotensin-converting
Performance of comorbidity scores to control for confounding in epidemiologic
enzyme inhibitors on mortality and morbidity in patients with heart failure. JAMA
studies using claims data. Am J Epidemiol 2001;154:854 – 864. 13. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of 2. The CONSENSUS Trial Study Group. Effects of enalapril on mortality in
classifying prognostic comorbidity in longitudinal studies: development and
severe congestive heart failure. N Engl J Med 1987;316:1429 –1435.
validation. J Chron Dis 1987;40:373–383. 3. The SOLVD Investigators. Effect of enalapril on survival in patients with 14. Hux JE, Ivis F, Flintoft V, Bica A. Diabetes in Ontario: determination of
reduced left ventricular ejection fractions and congestive heart failure. N Engl
prevalence and incidence using a validated administrative data algorithm. Dia-betes Care 2002;25:512–516. Simplified Peak Power Reserve in Patients With an Implantable Cardioverter-Defibrillator and Advanced Heart Failure
William T. Katsiyiannis, MD, Alan D. Waggoner, MHS, Benico Barzilai, MD,
Brian F. Gage, MD, MS, Jose M. Sanchez, MD, Joseph G. Rogers, MD,
Bruce D. Lindsay, MD, and Marye J. Gleva, MD
The prognostic ability of simplified peak power (SPP)
progressive pump failure as opposed to arrhythmic
reserve, a novel measure of left ventricular systolic
death. Contractile reserve determined by invasively
performance, was prospectively studied in patients
measured peak power has been used as a prognostic
with advanced heart failure (HF) and implantable
indicator in patients with Ventricular reserve
cardioverter-defibrillators. Reduced SPP reserve iden-
using noninvasive simplified peak power (SPP) is
tified patients who are at high risk for experiencing
easily obtained, afterload independent, can be preload
progressive HF. ᮊ2005 by Excerpta Medica Inc.
adjusted, and may add additional predictive power to
(Am J Cardiol 2005;95:286 –288)
traditional prognostic measures. We conducted a pro-spective study to determine whether noninvasive SPP
Some patients with left ventricular dysfunction and reserve can identify ICD candidates with rapidly pro-
ventricular arrhythmias derive limited benefit
gressive HF. Our hypothesis was that in patients with
from the placement of implantable cardioverter-defi-
ICDs in New York Heart Association functional class
brillators (ICDs), because they die of progressive
III HF, those with limited SPP reserve would have a
heart failure (HF). The accurate identification of this
greater number of adverse HF events.
group could guide the selection of patients who may
benefit from more directed HF therapy. Unfortunately,
We prospectively enrolled patients in New York
the tools that are currently available to stratify this
Heart Association class III HF who underwent ICD
population are imprecise. Patients with the most ad-
implantation for an American College of Cardiology–
vanced HF symptoms are more likely to die from
American Heart Association class I indication atBarnes-Jewish Hospital–Washington University School
From the Cardiovascular Division, Department of Internal Medicine,
of Medicine. Patients with either ischemic or nonisch-
Washington University School of Medicine, St. Louis, Missouri. Dr. Katsiy-
emic cardiomyopathy were included. Patients were ex-
iannis was supported by the Michael Bilitch fellowship of the North
cluded for the inability to complete a dobutamine stress
echocardiogram (i.e., the development of chest pain,
Massachusetts. Dr. Katsiyiannis’s address is: Minneapolis Heart Institute,
arrhythmia, or hypotension or hypertension necessitating
920 East Twenty-Eighth St., Suite 300, Minneapolis, Minnesota 55407. E-mail: [email protected]. Manuscript received June 2,
the early discontinuation of the study). A cohort of age-
2004; revised manuscript received and accepted September 8, 2004.
matched control patients without a history of HF or
2005 by Excerpta Medica Inc. All rights reserved.
The American Journal of Cardiology Vol. 95 January 15, 2005
TABLE 1 Characteristics of Patients With HF and ICDs
and where peak poweris equal to the product of peak aortic
flow and mean arterial pressure. Peakaortic flow was defined as the prod-
square of end-diastolic volume, anestimate of preload: (1) SPP reserve
SPP baseline; (2) SPP ϭ aortic flow ϫ mean arterial
pressure; (3) aortic flow ϭ aortic annulus area ϫ peak
aortic velocity; and (4) mean arterial pressure ϭ ([2 ϫ
systolic pressure] ϩ diastolic pressure)/3.
Patients were followed in the Washington Univer-
sity Medical Center Arrhythmia Clinic every 3months. At each follow-up visit, clinical informationwas obtained, including a history of shocks, ICDinterrogation, HF hospitalizations, or cardiac trans-plantation. Mortality data were collected from hospitalrecords and family interviews.
The composite end point of HF hospitalizations,
cardiac transplantation, and all-cause mortality wasanalyzed by the Kaplan-Meier method. Analyses wereperformed with SPP reserve dichotomized at 1.5W/ml2. This value was chosen a priori on the basis ofa previous Continuous variables were com-pared using the unpaired Student’s t test, and categor-
FIGURE 1. Kaplan-Meier curves for the composite end point in
ical variables were compared using Fisher’s exact test. patients with ICDs and New York Heart Association class III HF.
Analyses were performed using SPSS version 10.0 forWindows (SPSS, Inc., Chicago, Illinois) statisticalsoftware.
arrhythmia was also enrolled and underwent noninvasive
Twelve age-matched normal control patients un-
SPP reserve measurements only. The Human Studies
derwent dobutamine stress echocardiography and
Committee of Washington University School of Medi-
the determination of SPP reserve. Their mean age
cine approved all aspects of the study, and written in-
was 61 years. Their mean baseline ejection fraction
formed consent was obtained from all participants before
was 73 Ϯ 11%, and their mean SPP reserve was
35.2 Ϯ 19 W/ml2. Eighteen patients in New York
Dobutamine stress echocardiograms were performed
Heart Association class III HF who had ICDs were
beginning at an initial dose of 5 g · kgϪ1 · minϪ1 for 3
enrolled. Their mean age was 61 years. Their mean
minutes, followed by 10 g · kgϪ1 · minϪ1 for 3 min-
baseline ejection fraction was 32 Ϯ 11%, and their
utes, with subsequent dose increments of 10 g · kgϪ1 ·
mean SPP reserve was 3.5 Ϯ 3.2 W/ml2.
minϪ1 every 3 minutes, up to a maximum of 40 g ·
SPP reserve discriminated HF patients from con-
kgϪ1 · minϪ1. The infusions were discontinued when the
trols without overlap (mean 3.5, range 0.05 to 10.34 vs
patients achieved 85% of their target heart rate for their
mean 35.2, range 21.8 to 51.3, respectively; p
age group or if chest pain, ST-segment depression, or
Ͻ0.0001). The study population had a mean follow-up
new regional wall motion abnormalities developed.
of 15.5 months. There were no differences in the
Echocardiograms at rest and dobutamine stress echocar-
baseline characteristics of the 2 groups of patients
diograms were used to determine the left ventricular
with HF and ICDs: those with adequate (Ͼ1.5 W/ml2)
was 1 death, 1 heart transplantation, and 3 HF hospi-
predict survival in patients with ICDs and is not easily
talizations in the group with poor SPP reserve and no
measured in patients with more advanced HF and those
end points in the group with adequate SPP reserve.
There were 4 ICD shocks in the group with poor SPP
Therefore, an ideal prognostic tool would have the
reserve and 1 ICD shock in the group with adequate
predictive power of VO max, be noninvasive, and be
SPP reserve. Kaplan-Meier analysis of the composite
easy to use in patients with advanced HF. One such
end point of death, heart transplantation, or HF hos-
instrument that has emerged as a novel echocardio-
pitalization showed a significantly (p ϭ 0.02) greater
graphic measure of ventricular function is SPP re-
event rate in the group with poor SPP reserve
serve. It has an advantage over other echocardio-
SPP reserve discriminated the 2 groups of patients
graphic measures in that it is not significantly affected
with HF and ICDs without overlap, whereas the ejec-
by afterload, can be adjusted for and corre-
tion fraction showed considerable overlap. The mean
lates well with VO The present study demon-
SPP reserve of the group with death or transplantation
strates that SPP reserve identifies patients with ad-
was 0.63 Ϯ 0.4 W/ml2, and the mean SPP reserve of
vanced HF and ICDs who are more likely to have
the surviving patients was 4.9 Ϯ 2.3 W/ml2 (p ϭ
For ICDs to show a continued survival benefit in
patients with advanced HF, the risk for sudden cardiac
1. Marmor A, Schneeweiss A. Prognostic value of noninvasively obtained left ventricular contractile reserve in patients with severe heart failure. J Am Coll
death from life-threatening ventricular arrhythmias
must be sufficiently greater than the risk for dying
2. Armstrong GP, Carlier SG, Thomas JD. Estimation of cardiac reserve by peak
from other As ICD indications continue to
power: validation and initial application of a simplified index. Heart 1999;82:357–364.
expand, it is increasingly important to discriminate
3. Fogoros RN. Impact of the implantable defibrillator on mortality: the axiom of
patients who are less likely to die of HF, thus identi-
overall implantable cardioverter-defibrillator survival. Am J Cardiol 1996;
fying a subpopulation more likely to enjoy a survival
78(suppl):57A– 61A. 4. Rihal CS, Nishimura RA, Hatle LK. Systolic and diastolic function in patients
with clinical diagnosis of dilated cardiomyopathy: relation to symptoms and
The prognostic values of the left ventricular systolic
prognosis. Circulation 1994;90:2772–2779.
ejection fraction, mitral deceleration time, and serum
5. Xie GY, Berk MR, Smith MD. Prognostic value of Doppler transmitral flow patterns in patients with congestive heart failure. J Am Coll Cardiol 1994;24:
sodium concentration for mortality have been well es-
These measurements are insensitive and are
6. Lee WH, Packer M. Prognostic importance of serum sodium concentration and
relatively poor predictors of survival in patient with
its modification by converting enzyme inhibition in patients with severe chronicheart failure. Circulation 1986;73:257–267.
advanced HF. Peak oxygen consumption stress testing
7. Mancini DM, Eisen H, Kussmaul W. Value of peak exercise oxygen consump-
(VO max) has greater prognostic ability than the left
tion for optimal timing of cardiac transplantation in ambulatory patients with
ventricular ejection fraction and has been useful for the
heart failure. Circulation 1991;83:778 –786. 8.
risk stratification of ambulatory patients who may benefit
Sharir T, Feldman MD, Haber H. Ventricular systolic assessment in patients
with dilated cardiomyopathy by preload-adjusted maximal power. Validation and
noninvasive application. Circulation 1994;89:2045–2053. 288 THE AMERICAN JOURNAL OF CARDIOLOGYா
ACTA DA SESIÓN ORDINARIA CELEBRADA POLO PLENO MUNICIPAL O DÍA 29 DE NOVEMBRO DE 2.010. ACTA 10/10--------------------------------------------------------------No Concello de O PORRIÑO (PONTEVEDRA), no salón de sesións da casa consistorial, as 18 horas do día 29 de Novembro de 2.010, reúnese o Pleno da Corporación Municipal,baixo a presidencia do Sr. Alcalde ,Don JOSE NELSON SANTOS ARGIB
DATE REPORT ISSUED 22/03/2011 PLEASE FIND ENCLOSED OUR REPORT REFERENCE ALC E : 133257 : 0211BUREAU VERITAS CONSUMER PRODUCTS SERVICES UK LTD SAMPLE RETENTION POLICY Unless otherwise agreed in writing, samples will be retained for a minimum period of 28 days and then disposed of at BureauVeritas Consumer Products Services UK Ltd’s discretion. Bureau Veritas Consumer Products Serv
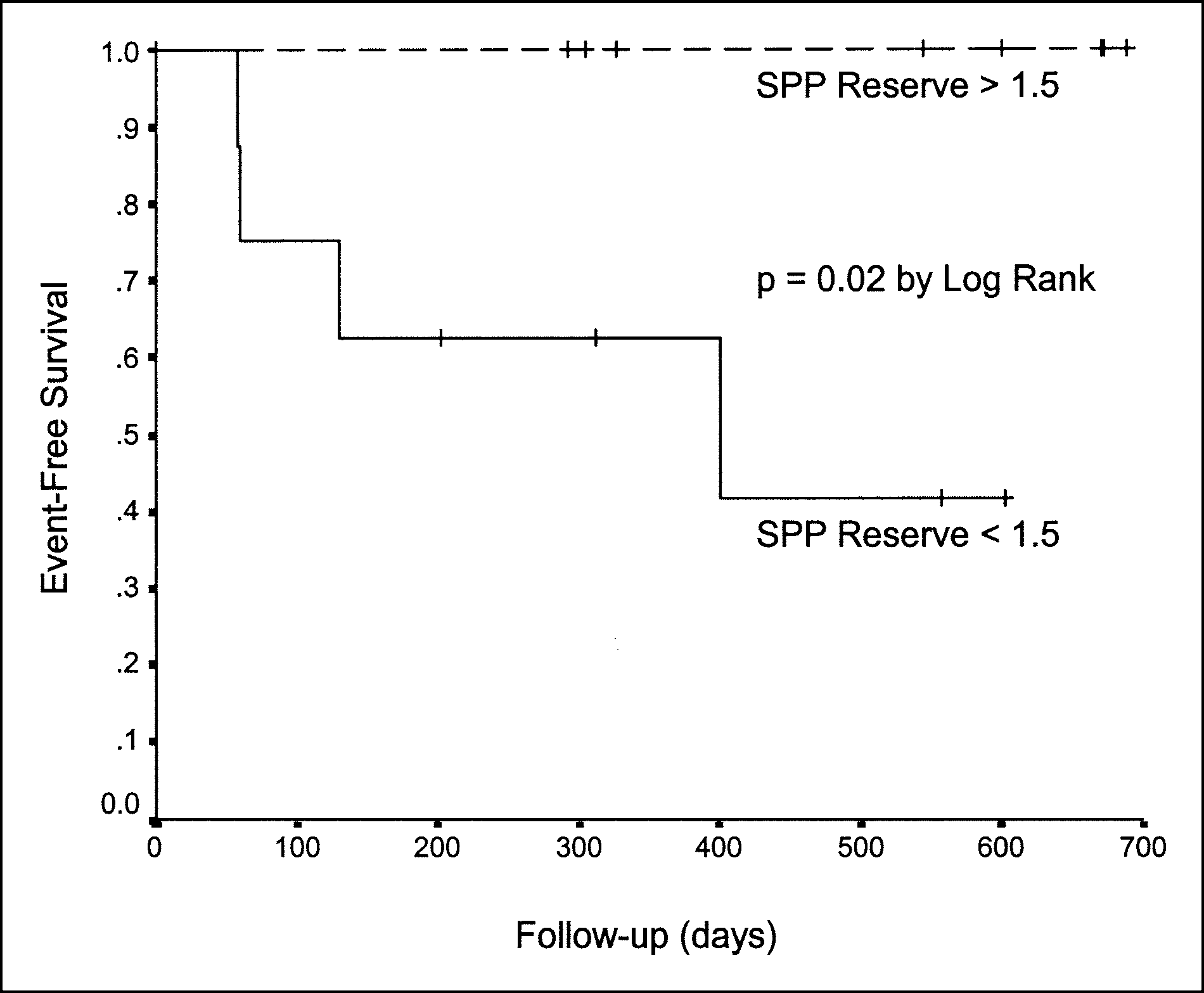 TABLE 1 Characteristics of Patients With HF and ICDs
TABLE 1 Characteristics of Patients With HF and ICDs