Assessment of Residual Periodontal Maintenance Populations
S.L. Campbell*, A.R. Biesbrock, R.W. Gerlach Procter & Gamble Co., Cincinnati, OH, USA ABSTRACT
Patients undergoing routine periodontal maintenance may Patients with moderate-to-severe disease often complete
present with residual disease. To evaluate residual disease initial care (scaling and root planing with or without surgery)
rates within a dental education setting, a random dental and then begin SPT with residual pocket depth. During SPT,
chart review was conducted involving a sample of patients in the overall clinical presentation is one of relative stability with a dental hygiene and a post graduate periodontal recall little gain or reduction in either pocket depths or attachment
maintenance program. Residual disease was characterized levels. However, some patients may continue to experience
• most recent periodontal therapy (date)
as the presence of one or more teeth (excluding third breakdown at individual sites (McFall 1982, Lindhe 1984,
molars) with at least one 6 mm pocket that bled on probing. Renvert 1990).
• disease severity (teeth with 5+ or 6+ mm pockets
In the post graduate periodontal maintenance (PPM)
sample, 29% of the patients (17/59) exhibited residual Because of this potential for residual and recurrent
periodontal disease. In contrast, 59% of the dental hygiene periodontitis, maintenance patients are at elevated risk for All abstracted data were entered directly into a spreadsheet
periodontal maintenance (DHPM) sample (13/22) had further breakdown, and as such, represent a "key group" for via laptop computer. Following data collection, cases were
residual disease. Patients with residual disease in both targeting care (Newman 1994). In this research, we categorized as to their probability of successfully passing
populations were similar with respect to mean age and evaluated dental maintenance behaviors and clinical status periodontal clinical trials entrance criteria at screening.
gender balance: mean age was 63.5 and 73.7 years in the of patients undergoing SPT within an academic dental
PPM and DHPM groups, respectively, while gender center. Specifically, the research was designed to compare
composition was 53% and 46% female in the PPM and
status among patients receiving SPT from the school's post
DHPM groups, respectively. Mean interval between graduate periodontics program versus those managed in the
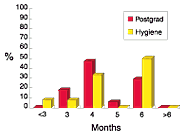
maintenance visits was similar in both groups, with 4.5 dental hygiene program.
A total of 81 patient charts were reviewed and abstracted: 59
months for PPM and 4.8 months for DHPM; however a
selected at random from the post graduate SPT program,
higher percentage of the PPM sample was seen on a shorter
and 22 selected at random from the dental hygiene SPT
maintenance interval ( >4 months ): 65% versus 45% in the
MATERIALS AND METHODS
program. Residual disease was characterized as the
DHPM group. These findings suggest that despite
presence of one or more teeth (excluding third molars) with
regular periodontal maintenance care, a significant To evaluate residual disease rates within a dental school at least one 6 mm pocket that bled on probing. percentage of patients in a dental education setting still setting, a random dental chart review was conducted presented with residual disease.
involving a sample of patients in a dental hygiene and a post The mean age of the collective sample was 67.1 years,
graduate SPT program. After obtaining permission from the ranging from 37 years to 88 years. Gender composition of
OBJECTIVE
school's institutional review board, the investigator the collective sample was evenly distributed, at 50.0%
assembled a random sample of patient charts from the two female. Patients with residual disease in both the post
The initial phase of periodontal care (surgical or non-
graduate (PPM) and dental hygiene (DHPM) populations
surgical) is typically followed by a maintenance phase of
were similar with respect to mean age and gender: mean
treatment, wherein supportive care including local scaling, Key data relevant to protocol eligibility criteria were age was 63.5 and 73.7 years respectively, while gender root planing and plaque removal is provided on a regular abstracted relating to demographics, clinical status and composition was 53% and 46% female in the PPM and basis, typically every 2-4 months (McFall 1989). This phase, dental utilization. No specific identifying information was DHPM groups, respectively. referred to as supportive periodontal therapy (SPT), collected (e.g., patient name). Where appropriate, dental represents an extension of the active phase of treatment radiographs were used to establish clinical status. In the PPM sample, 29% of the patients (17/59) exhibited
(McFall, 1989) where the primary objective is to achieve Abstracted variables included:
residual disease. In contrast, 59% of the DHPM sample
optimal patient plaque control by encouraging patient oral
hygiene and delivering frequent professional removal of plaque and calculus deposits (Ramjford 1987).
Research Presented at the 75th General Session of the IADR; Orlando, Florida March 19-23, 1997
Assessment of Residual Periodontal Maintenance Populations
S.L. Campbell*, A.R. Biesbrock, R.W. Gerlach Procter & Gamble Co., Cincinnati, OH, USA Table 1: Frequency Distribution of SPT Patients by Table 2: Frequency Distribution of SPT Patients by REFERENCES Number of Teeth With at Least One Periodontal Pocket Maintenance Interval
1. Lindhe J, Nyman S Long term maintenance of
patients treated for advanced periodontal disease. J Clin Periodontol 1984; 11:504-514.
2. McFall WT Tooth loss in 100 treated patients with
periodontal disease. A long-term study. J Periodontol 1982; 53:539-549.
3. McFall, WT Supportive treatment. from "American Academy of Periodontology. Proceedings of the World Workshop in Clinical Periodontics."
If these reported outcomes are representative, patients
Newman MG, Kornman KS, Doherty FM A 6-month multi-center evaluation of adjunctive tetracycline
undergoing periodontal maintenance in academic settings may present with residual periodontal disease. Importantly,
fiber therapy used in conjunction with scaling and
residual disease was more common among older patients,
root planing in maintenance patients: Clinical
The mean number of years since initial periodontal therapy especially those over age 60 years, and in some patients,
results. J Periodontol 1994, 65:685-691.
in the collective PPM and DHPM sample of 81 patients was involved most retained teeth.
5. Ramfjord SP Maintenance care for treated
9.5 years. Considering only patients with residual disease,
periodontitis patients. J Clin Periodontol
the mean number of years since initial therapy was 10.8
years and 6.7 years for the PPM and DHPM groups,
CONCLUSION
6. Renvert S, Nilvéus R, Dahlén G, Slots J, Egelberg
Regarding periodontal maintenance within dental
J. 5-year follow up of periodontal intraosseous
Mean interval between maintenance visits was similar in
school settings, these findings suggest:
defects treated by root planing or flap surgery. J
both groups, with 4.5 months for PPM and 4.8 months for
Clin Periodontol 1990;17:356-363.
DHPM; however a higher percentage of the PPM sample
-Dental school maintenance programs may include a
with residual disease were seen on a shorter maintenance
significant proportion of patients with residual
interval (< 4 months): 65% versus 45% in the DHPM group
-Differences may exist within dental schools as to disease severity and maintenance schedules for
patients in post graduate programs versus those in hygiene programs
-This pilot exercise using a convenience sample may be a useful model for identifying patient types within academic maintenance programs, and could potentially target enrollment and reduce overall clinical cycle time.
Research Presented at the 75th General Session of the IADR; Orlando, Florida March 19-23, 1997
Blackwell Science, LtdOxford, UKBCPBritish Journal of Clinical Pharmacology1365-2125Blackwell Publishing 2003573237243Review ArticlePeripheral vascular disease metabolic limitationsP. L. Greenhaff DOI:10.1111/j.1365-2125.2003.01989.x Metabolic inertia in contracting skeletal muscle: a novel approach for pharmacological intervention in peripheral vascular disease P. L. Greenhaff, S. P. Camp
Dental Drug Interacting Drug common examples Interaction Recommendation alcohol, antidipressants, opioids Possible additive CNS, respiratory limit maximum dose of LAs, CNS Depressants benbenzodiazipines, muscle relaxants, depression especially with opioids antipsychotics, antihistimines increased affect of vasoconstrictor Avoid vasoconstrictor with pati
 Assessment of Residual Periodontal Maintenance Populations
S.L. Campbell*, A.R. Biesbrock, R.W. Gerlach
Assessment of Residual Periodontal Maintenance Populations
S.L. Campbell*, A.R. Biesbrock, R.W. Gerlach 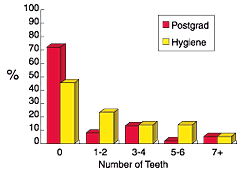
 Assessment of Residual Periodontal Maintenance Populations
S.L. Campbell*, A.R. Biesbrock, R.W. Gerlach
Assessment of Residual Periodontal Maintenance Populations
S.L. Campbell*, A.R. Biesbrock, R.W. Gerlach