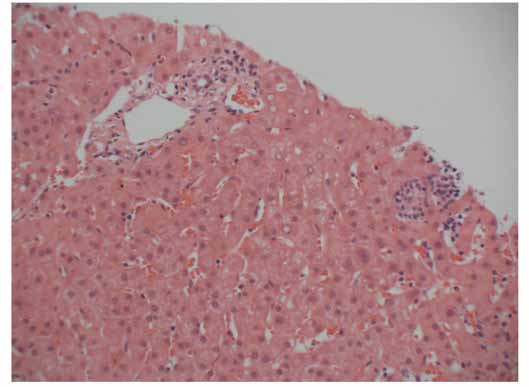
Gastroenterology Today 2007; 17(4) Metformin induced cholestatic hepatitis Dr. Emma Nixon1, Dr. A Simon2, Dr. G Lipscomb3, Dr. S Wells4 Introduction Figure 1. Liver Biopsy
Hepatic adverse drug reactions are common in everydayclinical practice. Most oral hypoglycaemic agents havebeen implicated in hepatotoxicity . While the sulphonureas,glucosidase inhibitors and the thiazolodineodines arecommonly reported to cause adverse reactions in the formof liver toxicity [1], there have been only three welldocumented reports of metformin induced hepatic injury[2-4]. This report describes a case of metformin inducedacute cholestatic hepatitis. Case report
A 58-year-old female was referred by her General Practi-tioner for investigation of jaundice. She gave a three week
Histological examination of the 1.9cm long core biopsy showed a
history of flu like symptoms, general fatigue and painless
normal lobular architecture with no fibrosis or portal inflammation.
jaundice. One week prior to the onset of symptoms she
There were small clusters of chronic inflammatory cells in the lobules,
had been started on metformin 500mg twice daily for newly
mild Kupffer cell hyperplasia and minimal macrovesicular fatty change.
Eosinophils were not prominent in the infiltrate. No spotty necrosis or
piecemeal necrosis was seen. There was no evidence of excess
haemosiderin, granulomata, alpha-one-antitrypsin bodies, excess
She was on no other regular medications. She had no
copper associated protein, bile stasis, bile ductile proliferation or
Mallory’s hyalin. The appearances were of mild lobular inflammation
significant past medical history. She reported no alcohol
and were thought to possibly represent resolving hepatitis. There were
excess, previous liver disease or jaundice, blood transfu-
no diagnostic features of autoimmune hepatitis.
sions, tattoos or travel abroad. Clinical examination wasunremarkable except for jaundice.
Laboratory investigations revealed a bilirubin of 52
Discussion
(normal <17umol/L), an aspartate aminotransferase (AST)level of 303 (normal <40U/L ), an alanine aminotrans-
This case represents one of the few reported incidents of
ferase (ALT) of 716 (normal <50U/L) and an alkaline phos-
metformin induced hepatitis. The time scale from the intro-
phatase (ALP) of 101 (normal <160IU/L). Her albumin was
duction of metformin to the onset of jaundice was four
42 and international normalised ratio 1.1. Serology for hep-
weeks. This is consistent with a drug reaction. The other
atitis A, B, C, E, CMV and EBV was negative. Autoimmune
reported cases documented hepatic injury occurring from
screen including anti-mitochondrial antibodies, anti-smooth
two to six weeks following institution of metformin. The liver
muscle antibodies, and anti-liver kidney microsomes was
biopsy showed normal liver architecture and features
of cholestasis and lobular inflammation. The histologicalfeatures were non specific and consistent with a drug
Results of abdominal ultrasonography revealed only mild
induced hepatitis. The patient was not taking any other
splenomegaly. A percutaneous liver biopsy showed
medications and other causes of acute hepatitis were
cholestasis with lobular inflammation, consistent with a
excluded. In previous reports the patients involved were
also taking other medications known to cause hepaticinjury, however in one of the three cases the metformin
Metformin was withdrawn and her liver function gradually
was reintroduced at a later date with a recurrence of the
improved. Her transaminitis resolved within three months
The reason for acute liver injury by metformin remainsunclear. Although metformin accumulates within the liver,it does not undergo hepatic metabolism and has not been
1. Clinical Fellow – Gastroenterology
shown to cause dose-dependent hepatotoxicity [5,6]. It
2. Staff Grade – Gastroenterology 3. Consultant – Gastroenterology
appears therefore to represent a rare idiosyncratic drug
4. Consultant – Histopathology
reaction, with resolution of hepatitis on its discontinuation. Royal Bolton Hospital , Bolton BL4 0JR
Gastroenterology Today 2007; 17(4)
The high prevalence of NASH related liver abnormalities in
2. Babich M, Pike J. Metformin induced acute hepatitis. Am J
patients with type 2 diabetes mellitus means that minor
Med. 1998; 104: 490-92.
elevation of liver enzymes are not uncommon in this
3. Desilets DJ, Shorr AF. Cholestatic jaundice associated with
population. This case highlights the importance of recog-
the use of metformin. Am J Gastroenterol. 2001;9 6: 2257-8.
nising drug induced hepatoxiticy in this group of patients,
4. Deutch M, Kountouras D. Metformin hepatotoxicity. Ann Int
in particular regard to metformin which is in wide clinical
. 2004; 140: 2025.
use and previously thought not to cause hepatic injury. 5. Wilcock C, Wyre ND. Subcellular distribution of metformin in
rat liver. J Pharmacol. 1991; 43(6): 442-4.
6. Scheen AJ. Clinical Pharmacokinetics of metformin. Clin
References
Pharmacokinet. 1996 May; 30(5): 359-71. Review.
1. Chittaii S, George J. Hepatatoxicity of commonly used drugs;
nonsteroidal anti-inflammatory dugs, antihypertensives, antidiabetic agents, anticonvulsants, lipid lowering agents, psychotropic drugs. Semin Liver Dis. 2002; 22: 169-83. Heart drugs may help people with bowel disorders
results of this preliminary research.
Statin drugs, widely prescribed toprevent heart disease may emerge
Technion develops world’s smallest medical
can enter a patient’s bloodstreamand deliver medical treatment.
fibrotic disease in their kidneys, but if
they’re taking statins, their condition
tend to improve,” said Dr. Burke. “We
Continued on next page . . . 109
University Medical Center Corporation Tucson, Arizona SUBJECT: Telemetry Management Policy: PM 90 Originator: Heidi Costello, Michelle Ziemba, Jayne Matte-Wilson, Gina Ragonese Responsible Person: Michelle Ziemba Effective Date: September 30, 2010 Revision Date: PURPOSE: To outline the nursing management of the telemetry monitored patient. SUPPORTIVE DATA: To pro
Biochemical and Biophysical Research Communications 275, 129 –133 (2000) doi:10.1006/bbrc.2000.3216, available online at http://www.idealibrary.com onChemotaxis and Biodegradation of 3-Methyl-4-Nitrophenol by Ralstonia sp. SJ98Bharat Bhushan,*,1 Sudip K. Samanta,*,2 Ashvini Chauhan,*Asit K. Chakraborti,† and Rakesh K. Jain*,3* Institute of Microbial Technology, Sector-39A, Chandigar
 Gastroenterology Today 2007; 17(4)
Gastroenterology Today 2007; 17(4)