Thorax 1999;54:278–281
Clinical presentation of exclusive cystic fibrosislung disease
Inez Bronsveld, Jan Bijman, Frauke Mekus, Manfred Ballmann, Henk J Veeze,Burkhard Tümmler
Abstract
child was born preterm with meconium ileus
The diagnosis of cystic fibrosis (CF) is
and died at day 10. The second child died dur-
based on the occurrence of two mutations in the cystic fibrosis transmembrane con-
suspected at necropsy. Our patient suVered
ductance regulator (CFTR) gene and on
from chronic nasal polyposis which had led to
assays that measure the basic defect of
13 polypectomies between the age of five and
abnormal chloride transport in the af-
23 years. By the age of 15 years she was referred
fected organs. However, in cases of atypi-
to a chest physician because of shortness of
cal CF not all diagnostic tests may be
breath during sports activity. Clubbing, sub-
positive. We present a patient with an
normal lung function, and decreased exercise
atypical CF phenotype in whom the only
tolerance were noted. The diagnosis of CF was
presenting symptom was severe CF-like
proposed because of the typical pulmonary
lung disease substantiated by an abnormal
manifestations but was discarded when normal
nasal potential diVerence. Genetic analy-
sweat electrolyte concentrations were found. sis showed that the patient was a sympto-
The diVerential diagnosis of allergy as the
matic heterozygote, which suggests that
underlying disease was excluded by normal IgE
one lesion in the CFTR gene may be suY-
skin prick tests and normal serum levels of spe-
cient to cause CF-like lung disease.
cific IgE. Immotile cilia syndrome was ex-
(Thorax 1999;54:278–281)
cluded by the normal microscopic appearanceof biopsy specimens of nasal cilia. Since
Keywords: cystic fibrosis; atypical cystic fibrosis; nasal
adolescence she had been underweight (below
3rd percentile) and had recurrent lower airway
Departments of Paediatrics and Cell
infections. Over the years increased sputum
Biology, Erasmus
Typical cystic fibrosis (CF) is caused by two
production and chronic cough became a clini-
University Rotterdam,
lesions in the cystic fibrosis transmembrane
cal problem. A lung biopsy specimen in 1984
Rotterdam,
conductance regulator (CFTR) gene which
showed a histological pattern consistent with
The Netherlands
give rise to a generalised exocrine disease of the
CF (bronchiectasis with localised purulent
respiratory, gastrointestinal, reproductive, and
bronchitis and surrounding fibrosis). Cultures
hepatobiliary tracts.1 The protein product of
of throat swabs or sputum were often positive
Department of
the CFTR gene is a chloride channel expressed
for Staphylococcus aureus (>90% of samples)
Neonatology, Sophia
in the apical membrane of epithelial cells2 so
but never for Pseudomonas aeruginosa. How-
Children’s Hospital,
diagnostic tests that measure the chloride con-
ever, the specific anti-P aeruginosa oprF IgG
Rotterdam,
ductance in exocrine epithelia—for example,
titre was positive, indicating that she had been
The Netherlands H J Veeze
the pilocarpine iontophoresis sweat test,3 intes-
exposed to P aeruginosa. Bronchodilators and
tinal current measurement (ICM),4 and nasal
intermittent antibiotics were prescribed but the
Department of
potential diVerence (NPD)5 6—have abnormal
patient generally discontinued medication after
Paediatrics and the
values in cases of typical CF. Atypical cases of
a few days, even during acute respiratory tract
Clinical CF Research
CF have a diVerent clinical presentation with
infections. At the age of 23 her lung function
Group, Medizinische
pancreatic suYciency, mild bronchitis, nasal
was reduced (vital capacity 1.5 l (48% pre-
Hochschule Hannover, D-30623 Hannover,
polyposis, congenital bilateral absence of the
dicted)), her chest radiograph had a Chrispin-
vas deferens (CBAVD), a borderline sweat test,
Norman score of 20, grade 3 (range 0–38), her
or ICM values which point to low residual
height was at the 25th percentile and weight
chloride secretion in intestinal tissue either by
below the 3rd percentile. However, her pancre-
CFTR or an alternative chloride channel.7–10
atic function was suYcient as shown by normal
We present a case characterised exclusively by
chymotrypsin levels in 1986, 1992, 1995, nor-
severe lung disease in whom other organs typi-
mal stool elastase levels (386 mg/g) in 1995,
cally involved in CF were not aVected and who
and by ultrasound investigation of the pan-
failed to show a defect in chloride transport.
enzymes or vitamin supplements. Serum levels
Patient history
of vitamins (vitamin A 370 µg/l, vitamin E
The 34 year old patient was the third child of
11 mg/l), bilirubin and liver enzymes were
Caucasian first generation cousins. The first
Exclusive cystic fibrosis lung disease
gel electrophoresis, blotting and hybridisationfollowed protocols 1, 5, 7, 8 and 9 of Bautsch etal.14 The intragenic CFTR haplotype was deter-mined for the sequence alterations T854T andM470V,15 16 the splice site polymorphism inintron 8 (TG) T ,11 17 and the microsatellites
NASAL POTENTIAL DIFFERENCE (NPD)NPD was measured using an adaptation of themethod described previously.5 In short, the nasalturbinate was superfused (1.7 ml/min) for peri-ods of three minutes with the following solutions(mol/l): saline to measure baseline PD; amilo-ride (10–4) to block Na+ channels; gluconate withamiloride to assess spontaneous Cl– conduct-ance; isoprenaline (10–4) in gluconate with ami-
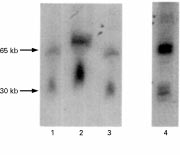
Autoradiogram of genomic ApaI digestionsprobed with CFTR cDNA (exon 7–24). No anomalous
loride to evaluate the presence of CFTR, and
band pattern is seen for the sample from the patient (lane
ATP (10–3) in isoprenaline/gluconate+amiloride
1). For comparison, lane 4 shows the probe reactive
solution to open non-CFTR Cl– channels. To
fragments from a specimen which carries a deletion in oneCFTR allele. ApaI cleaved fragments were separated in a
access the submucosal space a small needle (25
CHEF-DRTMII cell at 5.6 V/cm in 1% agarose gels (0.5
gauge) was inserted into the forearm and filled
TBE buVer, 10°C). Pulse times were linearly increased in
with saline. Both the needle and superfusion
two ramps from 5 to 20 s in 18 hours and from 5 to 90 s in20 hours.
catheter were connected to a high inputresistance voltage measuring device via salt
repetitive pilocarpine iontophoresis sweat tests
bridges and Ag/AgCl electrodes. The saline
performed since she was 11 years old the sweat
solution consisted of (mmol/l): NaCl (120), Na
electrolyte levels were always normal (range
(0.4), Na HPO (2.4). In the gluconate solution
NaCl was replaced by Na gluconate (145). Allsolutions were adjusted to pH 7.4. Methods This study was approved by the medical ethical committees of the Dutch and German partici-
pating hospitals and informed consent was
obtained from the patient. All chemicals were
described previously.4 Freshly obtained rectal
biopsy specimens were mounted in saline solu-
tion in the Ussing chamber (aperture 1.2 mm). After stabilising the basal short circuit current(I ) the tissue was exposed to the following
inhibitors and secretagogues (mol/l) to the
The promoter (–3.8 to –0.3 kb) and coding
mucosal (M) or serosal (S) side: glucose (10–2,
regions and the exon flanking intron sequences
M+S); amiloride (10–4, M); indomethacin
of the CFTR gene were screened for mutations
(10–5, M+S) to inhibit basal Cl– secretion by
by single strand conformation polymorphism
inhibiting the endogenous prostaglandin for-
(SSCP) analysis11 12 and, in the case of the
mation; carbachol (10–4, S), a Ca2+ linked
appearance of non-wild type band patterns in
secretagogue; forskolin (10–5, M+S) + 8-bromo
the high resolution SSCP gel, by subsequent
cyclic adenosine monophosphate (cAMP, 10–3,
sequencing.13 Deletions in the CFTR gene were
M+S) to open Cl– channels by activation of a
sought by repeated Southern hybridisations of
cAMP-dependent protein kinase and phospho-
rylation of specific membrane proteins; 4,4'-
probes encoding exon 1, exons 7–24, or the sec-
diisothiocyanatostilbene-2,2'-disulphonic acid
ond nucleotide binding fold (codons 1202–
(DIDS, 2.10–4, M) to inhibit Ca2+ dependent
1422). Preparation of unsheared genomic DNA
Cl– secretion; and histamine (5.10–4, S) to reac-
from fresh blood, complete restriction digestions
with ApaI, EagI, FspI, SalI or XhoI, pulsed field
Electrophysiological results for the study patient. Mean (SD) values for a controlgroup and a group of patients with CF are given for comparisonCFTR GENETICSDespite the familial consanguinity, the patient
was heterozygous at the CFTR locus which is
shown by the diVerent number of (TA) repeats
(n = 30, 34) for the microsatellite at the locus
IVS17bTA and her heterozygosity for a rare
the TG repeat with the T allele and the V470
CFTR isoform are known to decrease signifi-
cantly the amount and chloride channel activ-
ity of CFTR.16 After all CFTR exons and flank-
ing intron sequences and most of the promoter
decrease of 40%. Superfusion of gluconate in
the presence of amiloride resulted in a net
response of –3 mV, indicating subnormal Cl–conductance. With isoprenaline, which opens
CFTR Cl– channels, only a small response of
–4 mV was obtained which suggested that fewCFTR channels are present. No ATP response,
which is usually indicative of the presence of
alternative Cl– channels,20 was seen in the
In previous ICM studies carbachol has pro-
voked a negative reversed I in rectal tissue of
patients with CF, sometimes followed by a
positive residual response indicating the pres-
ence of residual Cl– secretion. In our patient the
Nasal potential diVerence (PD) measurements
ICM showed a Cl– secretory current in the
of the patient (x) and mean (SD) PD values of 25 controls
normal range on addition of carbachol (fig 3). (L) and 23 patients with CF ( ) following superfusion
DIDS, which inhibits the alternative pathway
with saline solution, amiloride (10–4 M) in saline solution,Cl– free solution with amiloride, isoprenaline (10–4 M) in
of Ca2+ activated Cl– currents, did not influence
Cl– free solution with amiloride, and ATP (10–3 M) in Cl–
the Cl– current, suggesting the presence of nor-
free solution with amiloride and isoprenaline.
mal CFTR mediated chloride conductance inthe intestine. Discussion The clinical and diagnostic features presented
by this case are conflicting in terms of the
expression of the basic defect in diVerent
tissues. In typical CF defective electrolyte
transport in the sweat gland, intestinal and air-
way epithelium is shown by a pathological out-
come of the sweat test, ICM and NPD. In ourcase, however, the sweat chloride concentrationand ion flow in the intestine were normal while
the NPD values were abnormally high. Patho-logically raised NPD values have so far only
been found in CF and not in any other lung
Measurements of intestinal current expressed as
disease with related clinical manifestations
changes in short circuit current (I ) of the patient (x) andmean (SD) I of 50 controls (L) and 51 patients with CF
syndrome, or congenital bronchiectasis.21 As
( ) following the addition of amiloride, carbachol, andexposure to 4,4'-diisothiocyanatostilbene-2,2'-disulphonic
well as a high baseline nasal PD, the patient’s
gluconate and isoprenaline response were alsoin the CF range. However, they do point to the
area up to –4 kb had been screened by SSCP,
presence of little residual CFTR Cl– permeabil-
one molecular lesion (the splice site consensus
ity in her respiratory epithelium. The clinical
transition 1898+3 A->G) was identified. A
symptoms of our patient, such as progressive
pancreatic insuYcient child with CF at our
obstructive bronchitis and bronchiectasis, spu-
clinic is homozygous for this condition and
tum production, and pathological bacterial
exhibited the typical pulmonary and gastro-
flora, are typical of CF and she has been
intestinal manifestations of CF indicating that
permanently on oxygen since the age of 30.
1898+3 A->G is a CF-causing lesion. No
This could explain her anorexic status since
anomalous bands were seen in autoradiograms
there is no sign of malabsorption or gastro-
of macrorestriction blots probed with CFTR
intestinal disease, as confirmed by normal vita-
cDNAs, indicating that the two CFTR alleles of
min A and E levels, pancreatic suYciency, and
our patient do not carry any major genomic
a normal ICM. This highly discordant expres-
sion of the basic defect in diVerent tissues isdescribed here for the first time: CFTR
function was unaVected in gastrointestinal tis-
On the day of electrophysiological investigation
sue whereas in airway tissue the abnormally
at the age of 32 she was underweight (below the
low Cl– conductance can only be accounted for
by defective epithelial Cl– transport. Other
17 kg/m2) and her lung function was severely
cases of CF with normal sweat test results and
pulmonary disease, as described for patients
1.23 l (38% predicted)). At this time she was
treated with continuous oxygen and showed
mutation,7 8 22 23 can clearly be diagnosed by an
severe clubbing. Electrophysiological measure-
abnormal ICM even when there are few or no
clinical signs of gastrointestinal involvement.10
presence of chloride conductance in her airway
The CFTR gene was screened for disease
and intestinal epithelium (table 1). The basal
causing lesions in all exons and flanking intron
NPD was –52 mV (fig 2). In the presence of
sequences and on one chromosome a sequence
amiloride the PD depolarised to –31 mV, a
alteration in a donor splice site was found
Exclusive cystic fibrosis lung disease
(1898+3 A->G). This sequence alteration was
4 Veeze HJ, Sinaasappel M, Bijman J, et al. Ion transport
first described in a compound heterozygous
abnormalities in rectal suction biopsies from children with cystic fibrosis. Gastroenterology 1991;101:398–403.
pancreatic suYcient patient (Ferrari et al, per-
5 Knowles MR, Carson JL, Collier AM, et al. Measurements
sonal communication) and was found also in a
of nasal transepithelial electrical potential diVerences innormal human subjects in vivo. Am Rev Respir Dis
pancreatic insuYcient CF patient homozygous
1981;124:484–90.
for this condition (see above). According to
6 Knowles MR, Paradiso AM, Boucher RC. In vivo nasal
potential diVerence: techniques and protocols for assessing
CFTR mutation analysis and the family anam-
eYcacy of gene transfer in cystic fibrosis. Hum Gene Ther
nesis, our patient is a carrier for one CFTR
1995;6:445–55.
mutation and hence should not express any CF
7 Gan KH, Veeze HJ, van den Ouweland AM, et al. A cystic
fibrosis mutation associated with mild lung disease. N Engl
symptoms. However, she carries an unfavour-
J Med 1995;333:95–9.
able combination of common intragenic poly-
8 Gilbert F, Li Z, Arzimanoglou I, et al. Clinical spectrum in
homozygotes and compound heterozygotes inheriting
morphisms. She is homozygous TG T for the
cystic fibrosis mutation 3849 + 10kb C > T: significance
for geneticists. Am J Med Genet 1995;58:356–9.
9 Kerem E, Rave-Harel N, Augarten A, et al. A cystic fibrosis
acceptor site, and the TG repeat together with
transmembrane conductance regulator splice variant with
the T stretch places the branch point nucle-
partial penetrance associated with variable cystic fibrosis
presentations. Am J Respir Crit Care Med 1997;
otide in an unfavourable position for splicing
155:1914–
leading to 30% of exon 9− CFTR transcript
10 Veeze HJ, Halley DJ, Bijman J, et al. Determinants of mild
clinical symptoms in cystic fibrosis patients. J Clin Invest 1994;93:461–6.
proteins that do not mature.16 24 Moreover, she
11 Dörk T, Mekus F, Schmidt K, et al. More than 50 diVerent
is homozygous for the V470 allele in exon 10.
CFTR mutations in a large group of German cystic fibrosis patients. Hum Genet 1994;94:533–42.
V470 CFTR proteins have a 1.7 fold decreased
12 Ravnik-Glavcak M, Glavcak D, Dean M. Sensitivity of sin-
intrinsic chloride channel activity compared
gle strand conformation polymorphism and heteroduplex method for mutation detection. Hum Mol Genet 1994;3:
with M470 CFTR proteins.16 These predispos-
ing polymorphisms in the intragenic back-
13 Zielenski J, Rozmahel R, Bozon D, et al. Genomic sequence
of the CFTR gene. Genomics 1991;10:214–28.
ground decrease the expression and function of
14 Bautsch W, Römling U, Schmidt KD, et al. Long-range
CFTR. Yet, they are present in both rectal and
restriction mapping of genomic DNA. In: Dear PH, ed. Genome mapping—a practical approach. Oxford: OxfordUniversity Press, 1997: 281–313.
unimpaired function of CFTR in the intestine
15 Dörk T, Neumann T, Wulbrand U, et al. Intra- and
while in the nasal tissue almost complete
extragenic marker haplotypes of CFTR mutations in cystic fibrosis families. Hum Genet 1992;88:417–25.
absence of Cl– conductance was found. How-
16 Cuppens H, Lin W, Jaspers M, et al. Polyvariant mutant
ever, the patient’s consanguineous descent
genes. J Clin Invest 1998;101:487–96.
leads to a genome-wide overrepresentation of
17 Teng H, Jorissen M, van Poppel H, et al. Increased
homozygous genotypes which may lead to fur-
proportion of exon 9 alternatively spliced CFTR transcriptin vas deferens compared with nasal epithelial cells. Hum
ther unfavourable combinations of factors that
Mol Genet 1997;6:85–90.
modify CFTR expression or lung function. As
18 Morral N, Estivill X. Multiplex amplification of three
gastrointestinal disease is not present, we
microsatellites within the CFTR gene. Genomics 1992;13: 1362–4.
propose that the genetic background predis-
19 Mekus F, Dörk T, Deufel T, et al. Analysis of microsatellites
poses to severe lung disease caused by tissue
by direct blotting electrophoresis and chemiluminescence detection. Electrophoresis 1995;16:1886–8.
specific regulatory elements which lead to the
20 Knowles MR, Clarke LL, Boucher RC. Activation by extra-
loss of CFTR function exclusively in the respi-
cellular nucleotides of chloride secretion in the airway epi-thelia of patients with cystic fibrosis. N Engl J Med
1991;325:533–8.
21 Knowles MR, Gatzy J, Boucher RC. Increased bioelectrical
potential diVerence across respiratory epithelia in cystic
This work was supported by the Deutsche Forschungsgemein-
fibrosis. N Engl J Med 1981;305:1489–95.
22 Dreyfus DH, Bethel R, Gelfand EW. Cystic fibrosis
3849+10kb C > T mutation associated with severe pulmo-
1 Welsh MJ, Tsui LC, Boat TF, et al. Cystic fibrosis. In: Scriver
nary disease and male fertility. Am J Respir Crit Care Med
CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic and
1996;153:858–60. molecular basis of inherited disease. New York: McGraw Hill,
23 Highsmith WE, Burch LH, Zhou Z, et al. A novel mutation
in the cystic fibrosis gene in patients with pulmonary
2 Bear CE, Li CH, Kartner N, et al. Purification and
disease but normal sweat chloride concentrations. N Engl J
functional reconstitution of the cystic fibrosis transmem-
Med 1994;331:974–80.
brane conductance regulator (CFTR). Cell 1992;68:809–
24 Strong TV, Wilkinson DJ, Mansoura MK, et al. Expression
of an abundant alternatively spliced form of the cystic
3 Gibson LE, Cooke RE. A test for concentration of
fibrosis transmembrane conductance regulator (CFTR)
electrolytes in sweat in cystic fibrosis of the pancreas utiliz-
gene is not associated with a cAMP-activated chloride con-
ing pilocarpine by iontophoresis. Pediatrics 1959;23:545–9.
ductance. Hum Mol Genet 1993;2:225–30.
USAGO: USA Gymnastics Magazine Online: Caffeine & Gymnastics Performance Caffeine & Gymnastics Performance By Dan Benardot, Ph.D., RD, LD Georgia State University USA Gymnastics National Team Nutritionist Not long ago, several coaches asked if having caffeine (by drinking a cup or more of coffee) before training or competition would improve performance. While this question is often as
Unique Research Journal of Medicine and Medical Sciences Vol. 1(4), pp. 031-033, October, 2013 Available online@http://www.uniqueresearchjournals.org/URJMMS Unique Research Journal of Medicine and Medical Sciences Dissociative disorder induced by topiramate in an obese young woman: A case report Omid Rezahosseini and Reza Bidaki* Rafsanjan University of Medical Sciences, Rafsanj
 Exclusive cystic fibrosis lung disease
gel electrophoresis, blotting and hybridisationfollowed protocols 1, 5, 7, 8 and 9 of Bautsch etal.14 The intragenic CFTR haplotype was deter-mined for the sequence alterations T854T andM470V,15 16 the splice site polymorphism inintron 8 (TG) T ,11 17 and the microsatellites
NASAL POTENTIAL DIFFERENCE (NPD)NPD was measured using an adaptation of themethod described previously.5 In short, the nasalturbinate was superfused (1.7 ml/min) for peri-ods of three minutes with the following solutions(mol/l): saline to measure baseline PD; amilo-ride (10–4) to block Na+ channels; gluconate withamiloride to assess spontaneous Cl– conduct-ance; isoprenaline (10–4) in gluconate with ami-
Autoradiogram of genomic ApaI digestions
probed with CFTR cDNA (exon 7–24). No anomalous
loride to evaluate the presence of CFTR, and
band pattern is seen for the sample from the patient (lane
ATP (10–3) in isoprenaline/gluconate+amiloride
1). For comparison, lane 4 shows the probe reactive
solution to open non-CFTR Cl– channels. To
fragments from a specimen which carries a deletion in oneCFTR allele. ApaI cleaved fragments were separated in a
access the submucosal space a small needle (25
CHEF-DRTMII cell at 5.6 V/cm in 1% agarose gels (0.5
gauge) was inserted into the forearm and filled
TBE buVer, 10°C). Pulse times were linearly increased in
with saline. Both the needle and superfusion
two ramps from 5 to 20 s in 18 hours and from 5 to 90 s in20 hours.
catheter were connected to a high inputresistance voltage measuring device via salt
repetitive pilocarpine iontophoresis sweat tests
bridges and Ag/AgCl electrodes. The saline
performed since she was 11 years old the sweat
solution consisted of (mmol/l): NaCl (120), Na
electrolyte levels were always normal (range
(0.4), Na HPO (2.4). In the gluconate solution
NaCl was replaced by Na gluconate (145). Allsolutions were adjusted to pH 7.4.
Exclusive cystic fibrosis lung disease
gel electrophoresis, blotting and hybridisationfollowed protocols 1, 5, 7, 8 and 9 of Bautsch etal.14 The intragenic CFTR haplotype was deter-mined for the sequence alterations T854T andM470V,15 16 the splice site polymorphism inintron 8 (TG) T ,11 17 and the microsatellites
NASAL POTENTIAL DIFFERENCE (NPD)NPD was measured using an adaptation of themethod described previously.5 In short, the nasalturbinate was superfused (1.7 ml/min) for peri-ods of three minutes with the following solutions(mol/l): saline to measure baseline PD; amilo-ride (10–4) to block Na+ channels; gluconate withamiloride to assess spontaneous Cl– conduct-ance; isoprenaline (10–4) in gluconate with ami-
Autoradiogram of genomic ApaI digestions
probed with CFTR cDNA (exon 7–24). No anomalous
loride to evaluate the presence of CFTR, and
band pattern is seen for the sample from the patient (lane
ATP (10–3) in isoprenaline/gluconate+amiloride
1). For comparison, lane 4 shows the probe reactive
solution to open non-CFTR Cl– channels. To
fragments from a specimen which carries a deletion in oneCFTR allele. ApaI cleaved fragments were separated in a
access the submucosal space a small needle (25
CHEF-DRTMII cell at 5.6 V/cm in 1% agarose gels (0.5
gauge) was inserted into the forearm and filled
TBE buVer, 10°C). Pulse times were linearly increased in
with saline. Both the needle and superfusion
two ramps from 5 to 20 s in 18 hours and from 5 to 90 s in20 hours.
catheter were connected to a high inputresistance voltage measuring device via salt
repetitive pilocarpine iontophoresis sweat tests
bridges and Ag/AgCl electrodes. The saline
performed since she was 11 years old the sweat
solution consisted of (mmol/l): NaCl (120), Na
electrolyte levels were always normal (range
(0.4), Na HPO (2.4). In the gluconate solution
NaCl was replaced by Na gluconate (145). Allsolutions were adjusted to pH 7.4.