M a x i m i z i n g L o c a l C o n t r o l a n d O r g a n P r e s e r v a t i o n i n S t a g e I V S q u a m o u s C e l l H e a d a n d N e c k C a n c e r W i t h H y p e r f r a c t i o n a t e d R a d i a t i o n a n d C o n c u r r e n t C h e m o t h e r a p y
By David J. Adelstein, Jerrold P. Saxton, Pierre Lavertu, Lisa A. Rybicki, Ramon M. Esclamado, Benjamin G. Wood,
Purpose: Results are reported from an aggressive curred in 51%. Despite feeding tube placement in 35 chemoradiotherapy protocol for advanced squamous patients (85%), the mean weight loss during chemora- cell head and neck cancer. diotherapy was 13.3% of initial body weight. One Patients and Methods: Patients with advanced patient died during treatment as a result of a pulmo- squamous cell head and neck cancer were treated with nary embolus. At a median follow-up period of 30 hyperfractionated radiation therapy (72 Gy at 1.2 Gy months, the 3-year Kaplan-Meier projected overall sur- twice per day) and two courses of concurrent chemo- vival was 59%, disease-specific survival 69%, likeli- therapy with fluorouracil (1,000 mg/m2/d) and cispla- hood of local control without surgical resection 91%, tin (20 mg/m2/d), both given as 96-hour continuous and local control with surgical resection 97%. The like- intravenous infusions during weeks 1 and 4 of radia- lihood of distant disease control at 3 years was 74%, tion therapy. Primary-site resection was reserved for and distant metastases were present in eight of 13 residual or recurrent primary-site disease after chemo- patients who died. radiotherapy. Neck dissection was considered for N2 Conclusion: This chemoradiotherapy schedule pro- or greater disease, irrespective of clinical response, and duces considerable but manageable toxicity. Survival for residual or recurrent neck disease after nonopera- and organ preservation are excellent for this poor- tive treatment. prognosis patient cohort. Distant metastases are the Results: Forty-one patients with stage IV disease most common cause of treatment failure. were treated. Toxicity was significant, with grade 3 to 4 J Clin Oncol 20:1405-1410. 2002 by American mucositis in 98%, dysphagia in 88%, and skin reaction Society of Clinical Oncology. in 85%. Neutropenic fever requiring hospitalization oc-
THE PROGNOSIS for patients with stage IV squamous been examined with evidence of increased efficacy when
cell head and neck cancer remains poor despite recent
compared with conventional daily fractionation. Recent
advances in multimodality management.1,2 Although pa-
data from a large randomized Radiation Therapy Oncology
tients may die as a result of distant metastatic disease, as a
Group trial suggest that there is an improvement in both
result of comorbid illness, or as a result of the development
locoregional control and disease-free survival from several
of a second primary neoplasm, the high frequency of local
or regional recurrence poses the greatest threat.2,3 These
These recent treatment innovations would be expected to
locoregional failures highlight the inadequacy of even the
most benefit patients with the most advanced locoregional
most aggressive multimodality treatments.
disease. At the Cleveland Clinic Foundation, we explored
During the past 20 years, systemic chemotherapy has
an aggressive treatment protocol that used hyperfractionated
been extensively tested in the management of this disease,
radiation therapy with concurrent fluorouracil and cisplatin
and many chemotherapeutic agents have been found to have
chemotherapy as definitive treatment for patients with
antineoplastic activity.1-3 The combination of fluorouracil
advanced squamous cell carcinoma of the head and neck.
and cisplatin remains the best-studied and most active drugregimen.4-6 One advantage of this drug combination is thatboth agents are radiosensitizers,7,8 and attempts to exploit this
From the Departments of Hematology and Medical Oncology,
property have been successful. Several recent randomized
Radiation Oncology, Otolaryngology and Communicative Disorders,
phase III studies have convincingly demonstrated both a
and Biostatistics, The Cleveland Clinic Foundation, Cleveland, OH.
survival and locoregional control benefit for concurrent radia-
Submitted June 29, 2001; accepted November 13, 2001.
tion and chemotherapy regimens with fluorouracil, cisplatin, or
Address reprint requests to David J. Adelstein, MD, Department of
both when compared with radiation therapy alone.9-14
Hematology and Medical Oncology, Desk R35, The Cleveland ClinicFoundation, 9500 Euclid Ave, Cleveland, OH 44195; email: adelstd@
Altered fractionation radiation therapy is another ap-
proach that has been studied in recent years in an effort to
2002 by American Society of Clinical Oncology.
improve locoregional control.15-17 Several schedules have
Journal of Clinical Oncology, Vol 20, No 5 (March 1), 2002: pp 1405-1410
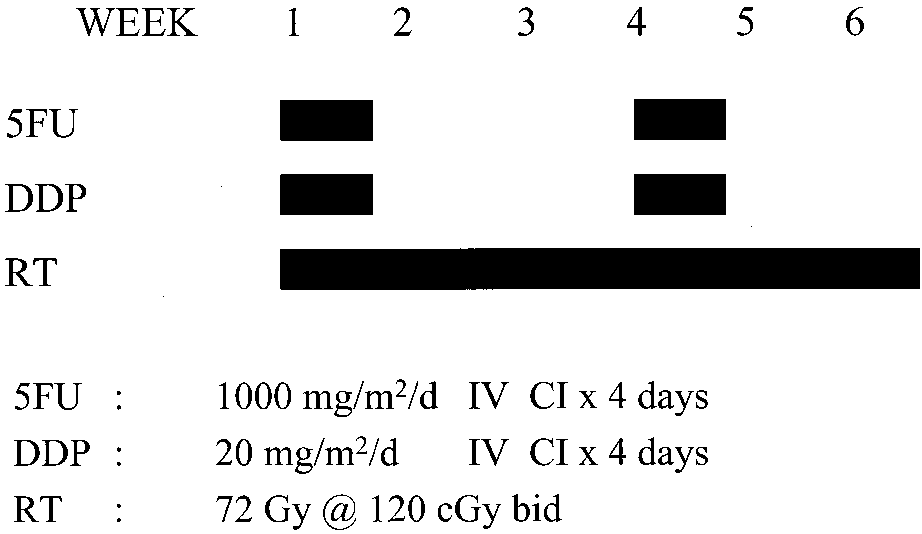
with a full course of hyperfractionated radiation therapy, 1.2 Gy twicedaily to a total dose of 72 Gy in 6 weeks. Concurrently, two courses ofchemotherapy with 4-day continuous infusions of fluorouracil (1,000mg/m2/d) and cisplatin (20 mg/m2/d) were given during weeks 1 and 4of radiation therapy.
At the Cleveland Clinic Foundation, patients receiving this chemo-
therapy regimen are hospitalized for hydration and antiemetic therapy. No chemotherapy dose modifications were made, irrespective of nadirblood counts or the blood count at the time of treatment, although thesecond course of chemotherapy was delayed until recovery if aneutropenic fever had developed. Peripheral intravenous catheters wereused for drug administration. Megavoltage radiotherapy was generatedby a 6-MV linear accelerator. Opposed lateral fields generally wereused with an electron beam boost given to selected lymph node regions
Fig 1. Treatment schema. 5FU, fluorouracil; DDP, cisplatin; RT, radiation
as indicated. There were no planned or toxicity-mandated breaks
therapy; IV CI, continuous intravenous infusion.
scheduled during the administration of the radiation therapy, nor werethere any toxicity-mandated delays in the administration of the second
We report our results in the subset of patients with the worst
prognosis, those with stage IV disease, and assess end
Patients were monitored at least weekly during their therapy in an
effort to manage treatment-induced side effects, particularly mucositis
points, including survival, locoregional control, and distant
and myelosuppression. Neutropenia with fever resulted in mandatory
metastatic disease control, in an effort to evaluate the effect
hospitalization and appropriate antibiotic therapy. Hospitalization was
also required when mucosal injury precluded an adequate oral intake. Percutaneous endoscopic gastrostomy feeding tubes were placed as
needed. Tracheostomies were performed in patients with significantly
Eligibility for this clinical trial required a diagnosis of stage III or IV
compromised airways, either at presentation or during the course of
squamous cell carcinoma of the head and neck. Patients with primary sites
in the nasopharynx, paranasal sinus, and salivary glands were excluded, as
Between 6 and 12 weeks after completion of definitive chemoradio-
were patients with metastatic disease involving neck but an unknown
therapy, a formal response analysis was undertaken. This analysis
primary site. Tumor and lymph node classifications were assigned accord-
included an examination made while the patient was anesthetized
ing to the 1992 staging system of the American Joint Committee on
(when clinically appropriate) and biopsy of any abnormalities sugges-
Cancer,19 and patients with hematogenous metastases (M1) disease were
tive of disease. A complete response required the disappearance of all
excluded. All patients were previously untreated and had an Eastern
clinical, radiographic, and, if applicable, pathologic evidence of dis-
Cooperative Oncology Group performance status of 0 or 1.
ease. Any response less than complete was considered to be a treatment
Pretreatment evaluation in all patients included a medical history, an
failure, and the patient underwent appropriate surgical resection if possible.
examination while the patient was anesthetized via panendoscopy, and
Primary-site resection was reserved for patients with histologically
a chest radiograph. Computed tomographic or magnetic resonance
verified residual primary-site disease after completing chemoradiother-
imaging scans of the involved head and neck region or other staging
apy. Neck dissection was performed if clinical evidence of residual
procedures for distant metastases were obtained if clinically indicated.
neck node disease was present after completion of nonoperative
Pretreatment laboratory evaluation included a complete blood cell
management. It was also recommended for patients with N2 or greater
count and serum chemistry tests, including urea nitrogen, creatinine,
disease at presentation, irrespective of clinical response, and for patients
calcium, phosphorous, alkaline phosphatase, AST, albumin, total pro-
undergoing primary-site resection. Salvage surgery was recommended for
tein, bilirubin, and uric acid. Adequate hematologic renal and hepatic
all patients if appropriate for local or regional disease recurrence.
function was required for the patient to enter the study. Patients with
After the completion of therapy, patients were observed by all
uncontrolled angina, active infection, or other uncontrolled malignancy
members of the multidisciplinary team. Careful clinical examination
was performed at 2- to 3-month intervals, and any suspected
All patients were deemed appropriate for initial nonoperative man-
locoregional or distant recurrence underwent biopsy. Radiographic
agement. Patients with gross bone involvement that was considered
studies were performed as clinically indicated. Survival times and
potentially resectable were not approached in this fashion; instead, theyunderwent definitive surgical resection. Similarly, patients with oral
times to specific events were calculated from the date radiation
cavity lesions for whom there was a significant risk of radiation damage to
therapy was initiated, and the results were analyzed as of March 1,
the mandible were also in general not offered this treatment approach.
2001. No patient was lost to follow-up study. The Kaplan-Meier
The study was approved and reviewed yearly by the Cleveland
method was used to estimate the events of interest, including overall
Clinic Foundation’s institutional review board. Written informed con-
survival, disease-specific survival, distant control, local control
sent was obtained from all patients before the initiation of treatment.
without surgery, and local control with surgery.20 Except for the
Patient care was provided by a multidisciplinary management team,
overall survival calculations, a patient was considered censored at
which included head and neck surgeons and medical, radiation, and
death if the event in question had not occurred. The patterns of
nurse oncologists. All patients underwent a pretreatment dental evalu-
failure analyses (local and distant control calculations) excluded the
ation with appropriate care, and all received a pretreatment audiogram.
single patient who died during treatment and who therefore could
The treatment schema is provided in Fig 1. All patients were treated
CHEMO RT FOR STAGE IV HEAD AND NECK CANCER
Table 1. Patient Characteristics (n ؍ 41) Table 3. Chemoradiotherapy Toxicity (n ؍ 41)
single toxic death as a result of a pulmonary embolusoccurred during treatment.
The median follow-up period for patients at risk was 30
months (range, 6 to 62 months). The Kaplan-Meier pro-jected overall survival at 2 years is 80% and at 3 years is
Between January 1996 and September 2000, 44 patients
59% (Fig 2). The projected disease-specific survival is 83%
with advanced squamous cell head and neck cancer were
at 2 years and 69% at 3 years (Fig 3), and this curve seems
enrolled onto this clinical trial. Forty-one of these patients
had stage IV disease at diagnosis and constitute the subject
Among the 40 patients assessable for pattern of disease
of this report. All patients were eligible, and all patients
failure, 39 experienced a complete response at the primary
were assessable for toxicity and survival. The clinical
site after chemoradiotherapy. The single patient with resid-
characteristics of these 41 patients and their tumors are
ual primary-site disease after chemoradiotherapy underwent
detailed in Table 1. Tumor and lymph node distribution is
successful salvage surgery, resulting in all 40 assessable
presented in Table 2. It should be noted that 35 (85%) of 41
patients achieving an initial local complete response. Two
patients had either T3 or T4 primary tumors and that 32
delayed local recurrences developed. In one, successful
patients (78%) were either T4 or N3 at presentation, confirm-
salvage resection was possible. Thus, among the 40 patients
ing the advanced locoregional disease present in this cohort.
assessable for pattern of failure, local control was achieved
The toxicity from this treatment was significant and is
without surgical resection in 37 and with surgical resection
detailed in Table 3. Grade 3 or 4 mucositis, dysphagia, and
in 39. Two of the three patients who experienced local
skin reaction occurred in almost all patients but were
persistence or recurrence received successful surgical sal-
reversible. Sixty-eight percent of patients experienced atleast one episode of neutropenia (Ͻ 1,000/mm3), and 21(51%) of the 41 patients required an unplanned hospitaliza-tion for management of neutropenic fever. Despite feedingtube placement in 35 (85%) of the 41 patients, the meanweight loss during treatment was 10.9 kg (range, 0 to 24.7kg), or 13.3% of initial body weight. Long-term feedingtube maintenance was required by only one patient. Renalinsufficiency was infrequent and entirely reversible. A
Table 2. Tumor (T) and Lymph Node (N) Distribution (n ؍ 41) Fig 2. Kaplan-Meier projected overall survival in stage IV patients. Fig 3. Kaplan-Meier projected disease-specific survival in stage IV Fig 5. Kaplan-Meier projected local control with surgery in stage IV patients. patients.
vage treatment. Figure 4 presents the Kaplan-Meier projec-
the 12 patients with clinical evidence of residual adenopa-
tion of local control without the need for surgery. This curve
thy. It should also be pointed out that among the nine N2,
plateaus at 91%. The local control rate is 97% if surgical
N3 patients who underwent neck dissection despite being
clinically free of neck disease, three (33%) proved to have
A clinical complete response was achieved in the neck in
residual pathologic evidence of cancer in the neck at the
24 of the 36 assessable patients with neck nodes identified
time of surgery. Among the entire patient cohort, only one
at presentation. Neck dissection was performed in 21 of the
patient experienced regional disease recurrence. This was a
34 patients with N2, N3 disease at diagnosis, including all
patient who initially presented with N3 disease and subse-
12 patients with residual palpable neck disease after che-
quently underwent a neck dissection for palpable and
moradiotherapy and nine of the 24 patients who achieved a
pathologically demonstrated disease persistence after che-
complete response in the neck. The results of neck node
moradiotherapy, who nonetheless experienced recurrence
management are detailed in Table 4. Thirteen of the 21
patients undergoing neck dissection had no residual evi-
Contrary to the usual pattern of failure, distant metastases
dence of disease in the neck. This included seven (58%) of
were relatively common, occurring in eight of the 40assessable patients. All eight died, including two whosubsequently developed hematogenous dissemination to thebrain. Thirteen of the 41 patients described herein havedied, including the eight who developed distant metastases,one patient who died during treatment, two patients whodied as a result of second primary aerodigestive tractmalignancies, and two who died as a result of comorbidillnesses. The patient with unresectable local disease recur-
Table 4. Neck Node Management (n ؍ 40) Fig 4. Kaplan-Meier projected local control without surgery in stage IV patients.
Abbreviation: CR, complete response.
CHEMO RT FOR STAGE IV HEAD AND NECK CANCER
rate of Յ 64% achieved in less advanced larynx/hypophar-ynx cancer after sequential chemotherapy and radiation,21,22suggesting an additional benefit from the concurrent treat-ment. The recently reported results from the Intergroupsecond-generation larynx preservation trial (Radiation Ther-apy Oncology Group 91-11) confirm this observation.23
Regional control proved more problematic. Residual
pathologic evidence of neck node disease was found in eightof the patients enrolled onto this trial, some of whom had noclinical evidence of residual cancer in the neck. Althoughthe majority of patients undergoing neck dissection in thisseries had no residual tumor at the time of surgery, we wereunable to accurately identify these patients preoperatively. We therefore continue to recommend neck dissection for allpatients with N2 or N3 disease at diagnosis, irrespective of
Fig 6. Kaplan-Meier projections of local control without surgery and
their clinical response after chemoradiotherapy, and in all
distant control in stage IV patients.
patients with residual clinical evidence of nodal involve-ment after nonoperative treatment.24
Even when a primary nonoperative treatment approach is
rence and the patient with regional disease recurrence both
chosen, the importance of ongoing surgical involvement in
died with distant metastases. This striking reversal in the
the management of these patients cannot be overstated. The
usual pattern of failure is illustrated in Fig 6. The projected
clinical evaluation of the primary site is often difficult after
likelihood of local control without surgery at 3 years is 91%
chemoradiotherapy, requiring repeated examinations while
compared with the projected 3-year likelihood of distant
the patient is anesthetized as well as multiple biopsies.
Similarly, the algorithms for neck management suggest theimportance of an ongoing surgical presence and a planned
neck dissection in appropriate patients if optimal treatment
Several important points emerge from this analysis. First,
results are to be achieved. Although the likelihood of organ
it is apparent that the toxicity of aggressive concurrent
preservation in this patient cohort is exciting, we cannot lose
chemotherapy and hyperfractionated radiation therapy is
sight of the fact that the overall treatment goal is cure. Surgical
significant. Almost all patients experienced severe mucosal
management remains important in the achievement of that end.
and skin toxicity, and more than half required hospitaliza-
These kinds of results, however, suggest that cure is a
tion for neutropenic fever. More important, however, was
reasonable and attainable goal, even in patients with ad-
the transient nature of this acute toxicity and the effective-
vanced locoregional tumors. Aggressive multimodality
ness of current supportive measures. No patient died as a
treatment strategies, with appropriate supportive care, by an
result of these treatment-related side effects. The single
experienced management team can produce a significant
toxic death reported resulted from a pulmonary embolus.
improvement in results when compared with historical
Aggressive follow-up care, early hospitalization and antibi-
experience. Although these patients may die for many
otic therapy for neutropenic fever, and prompt nutritional
reasons, the overwhelming cause of death in this cohort was
intervention with gastrostomy placement was critical in
distant metastatic disease, not locoregional tumor, comor-
maintaining the dose intensity of this treatment regimen and
bidity, or second primary neoplasms. Other investigators
was in large part responsible for the success achieved.
who used similar aggressive locoregional treatments have
Although the toxicity encountered was formidable, it was
made this same observation,25 and attention must now be
manageable and would seem justifiable given these results.
focused on the prevention of these distant metastases.
Future attention will be directed to the potential long-term
Interventions might include the use of additional multiagent
toxicities that may develop in this patient cohort.
chemotherapy given as either induction or adjuvant treat-
Second, despite the initial presentation with advanced
ment, or the use of other, nonchemotherapeutic systemic
locoregional tumors, local control of disease was excellent.
approaches. The complexity of these treatment regimens
Organ preservation, or local control without the need for
and the effect on patient compliance remain a significant
surgical resection, was possible in 91% of these stage IV
concern. Similar attention should also be directed toward
patients. One can contrast this with the organ preservation
possible toxicity modification, if this can be accomplished
without a compromise in overall treatment results. Initial
experienced supportive care team. The survival, local con-
efforts with agents such as amifostine26 and pilocarpine27
trol, and organ preservation were excellent despite the
advanced stage of these patients at diagnosis. Distant
We conclude that this chemoradiotherapy schedule pro-
metastases have now become the most common cause of
duces considerable toxicity and requires management by an
treatment failure at our institution.
1. Dimery IW, Hong WK: Overview of combined modality thera-
14. Brizel DM, Albers ME, Fisher SR, et al: Hyperfractionated
pies for head and neck cancer. J Natl Cancer Inst 85:95-111, 1993
irradiation with or without concurrent chemotherapy for locally ad-
2. Adelstein DJ, Tan EH, Lavertu P: Treatment of head and neck
vanced head and neck cancer. N Engl J Med 338:1798-1804, 1998
cancer: The role of chemotherapy. Crit Rev Oncol Hematol 24:97-116,
15. Ang KK: Altered fractionation trials in head and neck cancer.
3. Vokes EE, Weichselbaum, RR, Lippman SM, et al: Head and
16. Mendenhall WM, Parsons JT: Altered fractionation in radiation
neck cancer. N Engl J Med 328:184-194, 1993
therapy for squamous-cell carcinoma of the head and neck. Cancer
4. Forastiere AA, Metch B, Schuller DE, et al: Randomized com-
parison of cisplatin plus fluorouracil and carboplatin plus fluorouracil
17. Hu KS, Harrison LB: Altered fractionation in the treatment of
versus methotrexate in advanced squamous-cell carcinoma of the head
head and neck cancer. Curr Oncol Rep 1:110-123,1999
and neck: A Southwest Oncology Group study. J Clin Oncol 10:1245-
18. Fu KK, Pajak TF, Trotti A, et al: A Radiation Therapy Oncology
Group (RTOG) phase III randomized study to compare hyperfraction-
5. Jacobs C, Lyman G, Velez-Garcia, et al: A phase III randomized
ation and two variants of accelerated fractionation to standard fraction-
study comparing cisplatin and fluorouracil as single agents and in
ation radiotherapy for head and neck squamous cell carcinomas: First
combination for advanced squamous cell carcinoma of the head and
report of RTOG 9003. Int J Radiat Oncol Biol Phys 48:7-16, 2000
19. Beahrs OH, Henson DE, Hutter RVP (eds): Manual for Staging
6. Adelstein DJ: Induction chemotherapy in head and neck cancer.
of Cancer (ed 4). Philadelphia, PA, Lippincott, 1992
Hematol Oncol Clin North Am 13:689-698, 1999
20. Kaplan EL, Meier P: Nonparametric estimation of incomplete
7. Vietti T, Eggerding F, Valeriote F: Combined effect of x-
observations. J Am Stat Assoc 53:457-481, 1958
radiation and 5-fluorouracil on survival of transplanted leukemic cells.
21. Wolf GT, Hong WK, Fisher SG, et al: Induction chemotherapy
plus radiation compared with surgery plus radiation in patients with
8. Douple EB: Platinum-radiation interactions. Natl Cancer Inst
advanced laryngeal cancer. N Engl J Med 324:1685-1690, 1991
22. Lefebvre JL, Chevalier D, Luboinski B, et al: Larynx preserva-
9. Jeremic B, Shibamoto Y, Stanisavljevic B, et al: Radiation
tion in pyriform sinus cancer: Preliminary results of a European
therapy alone or with concurrent low-dose daily either cisplatin or
Organization for Research and Treatment of Cancer phase III trial.
carboplatin in locally advanced unresectable squamous cell carcinoma
of the head and neck: A prospective randomized trial. Radiother Oncol
23. Forastiere AA, Berkey B, Maor M, et al: Phase III trial to
preserve the larynx: Induction chemotherapy and radiotherapy versus
10. Jeremic B, Shibamoto Y, Milicic B, et al: Hyperfractionated
concomitant chemoradiotherapy versus radiotherapy alone, Intergroup
radiation therapy with or without concurrent low-dose daily cisplatin inlocally advanced squamous cell carcinoma of the head and neck: A
Trial R91-11. Proc Am Soc Clin Oncol 20:2a, 2001 (abstr 4)
prospective randomized trial. J Clin Oncol 18:1458-1464, 2000
24. Lavertu P, Adelstein DJ, Saxton JP, et al: Management of the
11. Adelstein DJ, Adams GL, Li Y, et al: A phase III comparison of
neck in a randomized trial comparing concurrent chemotherapy and
standard radiation therapy (RT) versus RT plus concurrent cisplatin
radiotherapy with radiotherapy alone in resectable stage III and IV
(DDP) versus split-course RT plus concurrent DDP and 5-fluorouracil
squamous cell head and neck cancer. Head Neck 19:559-566, 1997
(5FU) in patients with unresectable squamous cell head and neck
25. Vokes EE, Kies MS, Haraf DJ, et al: Concomitant chemoradio-
cancer (SCHNC): An Intergroup study. Proc Am Soc Clin Oncol
therapy as primary therapy for locoregionally advanced head and neck
12. Adelstein DJ, Saxton JP, Lavertu P, et al: A phase III random-
26. Brizel DM, Wasserman TH, Henke M, et al: Phase III random-
ized trial comparing concurrent chemotherapy and radiotherapy with
ized trial of amifostine as a radioprotector in head and neck cancer.
radiotherapy alone in resectable stage III and IV squamous cell head
and neck cancer: Preliminary results. Head Neck 19:567-575, 1997
27. Scarantino CW, LeVeque FG, Scott CB, et al: A phase III study
13. Wendt TG, Grabenbauer GG, Rodel CM, et al: Simultaneous
of concomitant oral pilocarpine to reduce hypo-salivation and mucosi-
radiochemotherapy versus radiotherapy alone in advanced head and
tis associated with curative radiation therapy in head and neck cancer
neck cancer: A randomized multicenter study. J Clin Oncol 16:1318-
patients: RTOG 9709. Proc Am Soc Clin Oncol 20:225a, 2001 (abstr
Fire Resistant Insulated Glass - SYSTEMGLAS ® Doors Fire Doors within All Glass Screens: Single & Double Leaf (1) SYSTEMGLASfi Door 30 & 60 Minutes Fire Rating SYSTEMGLAS® Doors are constructed without any visible glazingbeads on the retaining frame. It can be built as single or double-leafdoor in a SYSTEMGLAS® screen or solid wall element. A choice offloor or head mo
Monday, December 13, 2010 at 11 a.m. IGBMC Auditorium Special Seminar Transcriptional Regulation of Adipogenesis and Energy Homeostasis Bruce SPIEGELMAN Dana Farber Cancer Institute, Harvard Medical School, BOSTON - USA The nuclear receptor PPARγ is the dominant regulator of fat cell differentiation and development. Expression and agonist activation of PPARγ is suffic
 with a full course of hyperfractionated radiation therapy, 1.2 Gy twicedaily to a total dose of 72 Gy in 6 weeks. Concurrently, two courses ofchemotherapy with 4-day continuous infusions of fluorouracil (1,000mg/m2/d) and cisplatin (20 mg/m2/d) were given during weeks 1 and 4of radiation therapy.
with a full course of hyperfractionated radiation therapy, 1.2 Gy twicedaily to a total dose of 72 Gy in 6 weeks. Concurrently, two courses ofchemotherapy with 4-day continuous infusions of fluorouracil (1,000mg/m2/d) and cisplatin (20 mg/m2/d) were given during weeks 1 and 4of radiation therapy.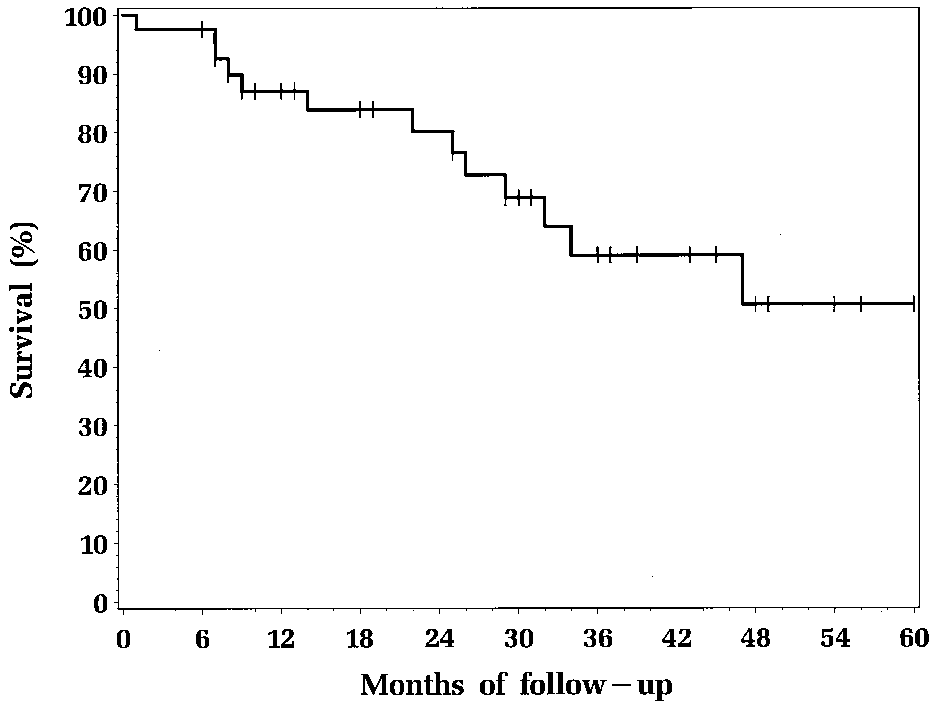 CHEMO RT FOR STAGE IV HEAD AND NECK CANCER
Table 1. Patient Characteristics (n ؍ 41)
CHEMO RT FOR STAGE IV HEAD AND NECK CANCER
Table 1. Patient Characteristics (n ؍ 41)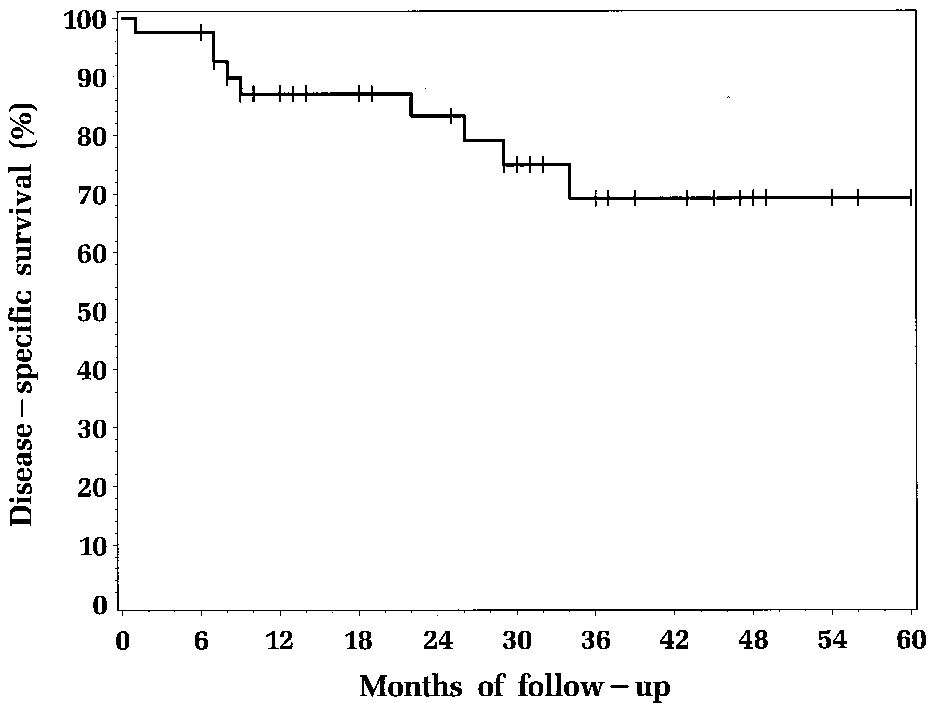
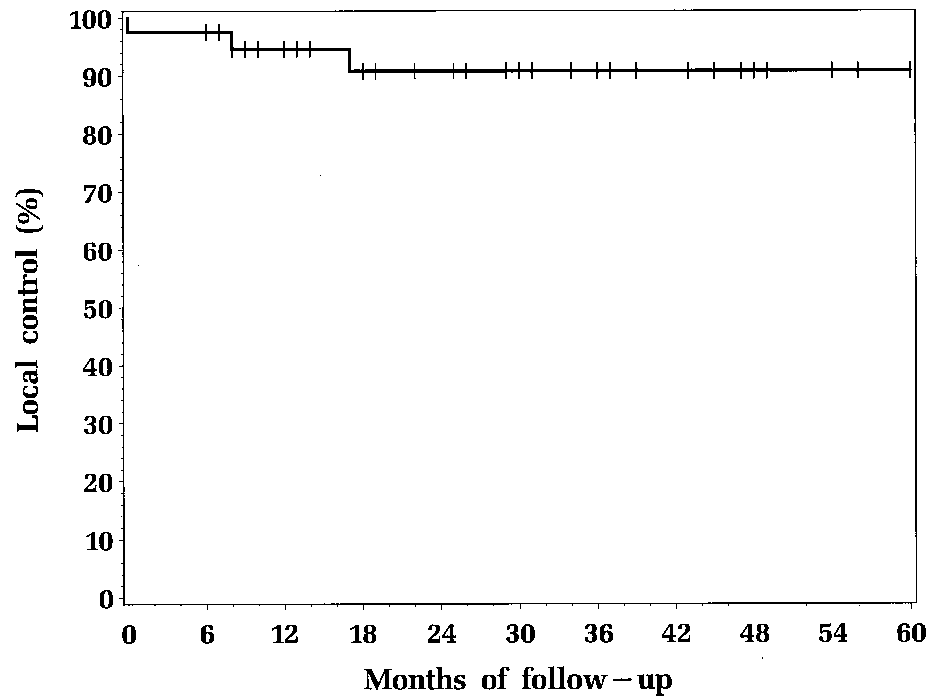
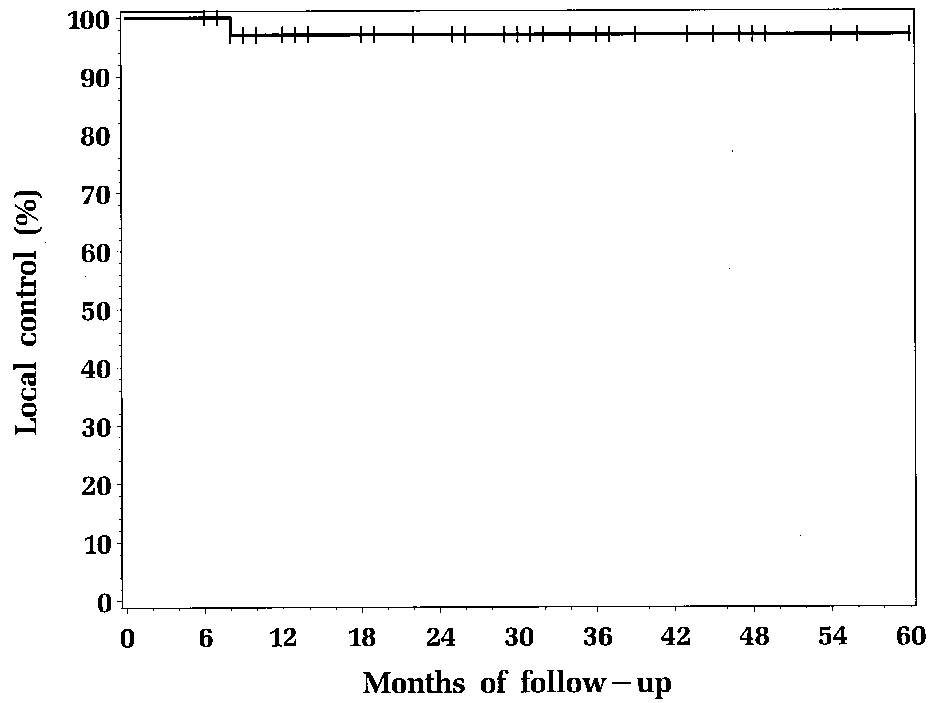 Fig 3. Kaplan-Meier projected disease-specific survival in stage IV
Fig 3. Kaplan-Meier projected disease-specific survival in stage IV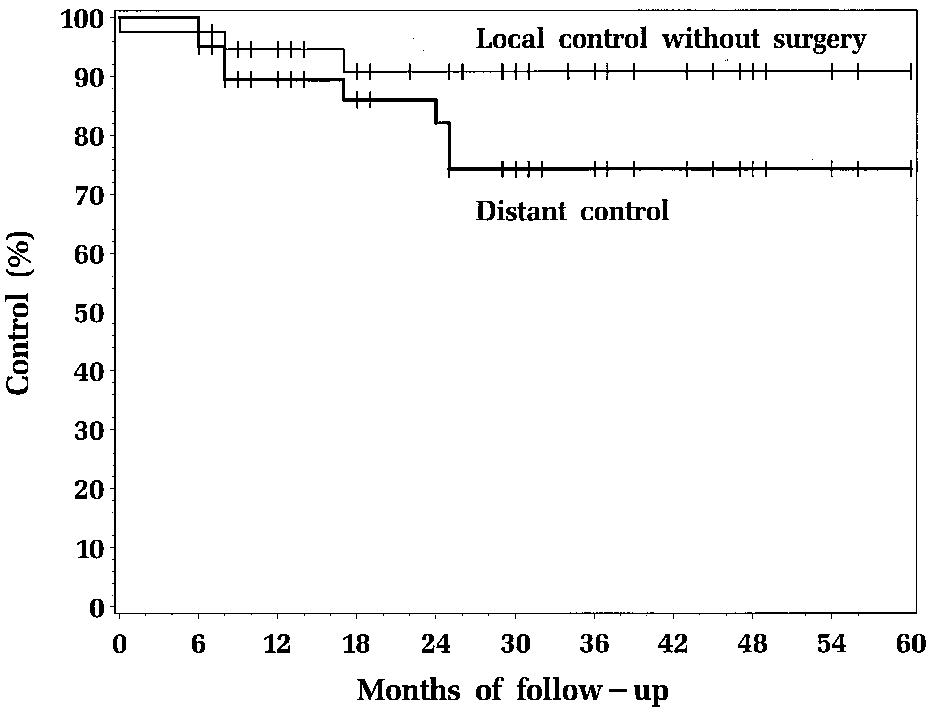 CHEMO RT FOR STAGE IV HEAD AND NECK CANCER
rate of Յ 64% achieved in less advanced larynx/hypophar-ynx cancer after sequential chemotherapy and radiation,21,22suggesting an additional benefit from the concurrent treat-ment. The recently reported results from the Intergroupsecond-generation larynx preservation trial (Radiation Ther-apy Oncology Group 91-11) confirm this observation.23
Regional control proved more problematic. Residual
pathologic evidence of neck node disease was found in eightof the patients enrolled onto this trial, some of whom had noclinical evidence of residual cancer in the neck. Althoughthe majority of patients undergoing neck dissection in thisseries had no residual tumor at the time of surgery, we wereunable to accurately identify these patients preoperatively.
CHEMO RT FOR STAGE IV HEAD AND NECK CANCER
rate of Յ 64% achieved in less advanced larynx/hypophar-ynx cancer after sequential chemotherapy and radiation,21,22suggesting an additional benefit from the concurrent treat-ment. The recently reported results from the Intergroupsecond-generation larynx preservation trial (Radiation Ther-apy Oncology Group 91-11) confirm this observation.23
Regional control proved more problematic. Residual
pathologic evidence of neck node disease was found in eightof the patients enrolled onto this trial, some of whom had noclinical evidence of residual cancer in the neck. Althoughthe majority of patients undergoing neck dissection in thisseries had no residual tumor at the time of surgery, we wereunable to accurately identify these patients preoperatively.