Clinical Endocrinology (2005) 63, 530–536 Adaptation of the hypothalamic-pituitary hormones during intensive endurance training
T. Bobbert*†, L. Brechtel¶, K. Mai*†, B. Otto‡, C. Maser-Gluth§, A. F. H. Pfeiffer*†, J. Spranger*† and S. Diederich**
*Department of Endocrinology, Diabetes and Nutrition, Charité University Medicine Berlin, Campus Benjamin Franklin, Berlin, †Department of Clinical Nutrition, Germany Institute of Human Nutrition Potsdam, Nuthetal, ‡Medical Department, University Hospital Innenstadt, Munich, §Steroid Laboratory, Department of Pharmacology, University of Heidelberg, Heidelberg, ¶Department of Sports Medicine, Humboldt University Berlin, Berlin, Germany, **Endokrinologikum Berlin, Centre for Endocrine and Metabolic Diseases Berlin, Germany
(Received 18 April 2005; returned for revision 1 June 2005; finally
revised 7 June 2005; accepted 25 August 2005)
Objective Physical activity leads to changes in the hypothalamic- pituitary hormonal system. However, acute and long-term adaptations have not yet been precisely characterized. In this study, the changes of the hormonal system as a result of marathon training and running Introduction
a marathon were examined. In particular, we focused on adaptations
Physical activity is known to induce various endocrine changes1,2
of the hypothalamic-pituitary-adrenocortical (HPA) axis, regarding
such as an activation of the hypothalamic-pituitary-adrenocortical
the activation or inactivation of cortisol to cortisone by the 11β-
(HPA) system3–5 but varies between acute and long-term adapta-
hydroxysteroid-dehydrogenase system (11β-HSD).
tions.6 In particular, relatively short-term intensive physical activity
Design Patient measurements: 8 healthy women and 11 healthy
leads to increased plasma levels of glucocorticoids like cortisol. This
men volunteered for this study. Blood samples, 24-h urine and a
is apparently required to cope with the higher demand of energy as
dexamethasone suppression test were analysed for metabolic
a result of the acute stress, e.g. running a marathon.7 Data concerning
and hormonal parameters at five different dates 12 weeks around
long-term physical activity or endurance training are not conclusive.
In some studies it was suggested that chronic stress or physical training
Results Cortisol and ACTH values decreased significantly 2 days
leads to a pseudo-Cushing’s syndrome with elevated cortisol levels
after the marathon, whereas the activity of the whole body 11β-HSD-1
or insufficient suppression in the dexamethasone suppression test.8,9
was up-regulated. An increased suppression of cortisol levels was
On the other hand there are also studies that showed a decrease in
observed in the dexamethasone suppression test after 6 weeks of
cortisol levels after long-term endurance training or competition.10,11
reduced training levels. Ghrelin was elevated 2 days after the marathon.
Furthermore, in some studies no changes in cortisol metabolism
Only minor changes in the other hypothalamic-pituitary-hormonal
were found.12 In addition to the mechanism of the cortisol synthesis
axes could be observed. However, the free androgen index increased
or production in response to exercise, there is no information about
significantly after 6 weeks of reduced training.
the activation or inactivation of cortisol to its inactive metabolite,
Conclusions The HPA system appeared to become chronically
cortisone, by the 11β-hydroxysteroid-dehydrogenase system (11β-
activated by continuous physical training and therefore less sensitive
HSD).13,14 The NADP+/ H-dependent 11β-HSD type 1 (11β-HSD-1)
to the dexamethasone suppression test. The acute stress of the mar-
enzyme functions in vitro as a bidirectional oxidoreductase and
athon led to a central exhaustion of the HPA system with a paracrine
is expressed ubiquitously. In vivo, 11β-HSD-1 acts mainly as a
counteraction by the activation of the 11β-HSD system. Changes in
reductase and activates inactive cortisone to cortisol. Thereby it is
the other hypothalamic-pituitary hormonal axes were the result of
believed that 11β-HSD-1 modulates intracellular concentrations of
long-term differences in training levels and were not altered by the
active glucocorticoids and occupancy of the glucocorticoid-receptor.
The main function of 11β-HSD-2 is the protection of the unselectivemineralocorticoid receptor, which has similar affinity to cortisol andaldosterone. This isoenzyme converts large amounts of cortisol toinactive cortisone, thus allowing the less concentrated aldosterone
Correspondence: Thomas Bobbert, Department of Endocrinology, Diabetes
to bind to the mineralocorticoid receptor.
and Nutrition, Charité University Medicine Berlin, Campus Benjamin
Besides the changes in glucocorticoid secretion and metabolism
Franklin, Hindenburgdamm 30, 12200 Berlin, Germany. Tel.: +4930/8445 4125; Fax: +4930/8445 4204. E-mail: [email protected]
following physical activity, the response of other hypothalamic-pituitary
Endurance training and pituitary hormones
hormones to endurance training are still not clear. The changes
C-reactive protein (CRP). The volunteers received 1 mg dexametha-
in the growth hormone /insulin-like growth factor-I (GH / IGF-I)
sone, which they were asked to take at 12:00 h on the same day. At
axis as a result of endurance training seem to depend on many
8:00 h of the second day, blood samples were taken for cortisol and
factors. Short-term activity leads to an increase of GH, IGF-1 and
IGF-BP3,15,16 whereas there is little information about chronic phys-ical activity. In elderly men, no differences in IGF-I, GH and IGF-
BP3 levels were found between endurance-trained and normal men. However, IGF-BP1/2 levels were slightly different in both groups.17
After sampling in ethylenediaminetetraacetic acid or serum tubes,
A recently discovered hormone, with strong GH-releasing prop-
blood was immediately chilled on ice and centrifuged; aliquots were
erties, is ghrelin.18 Ghrelin, a 28-amino acid peptide, is produced by
frozen at −20 °C until assayed. Blood samples were analysed for cor-
the enterocrine cells of the gastric mucosa. It is the natural ligand
tisol, ACTH, testosterone, SHBG, LH, FSH, IGF-1, IGF-BP3, TSH,
of GH secretagogue receptor and stimulates GH secretion more
fT4 by the full automatic chemiluminiscence-immunoassay system
potently than GH-releasing hormone (GHRH).19 In addition, ghrelin
IMMULITE from DPC Biermann (Bad Nauheim, Germany). Free
also stimulates the release of corticotropin releasing hormone
androgen index was calculated by FAI = testosterone × 100/SHBG.
(CRH), vasopressin, ACTH, cortisol, prolactin and aldosterone,19–21
CRP was measured with COBAS MIRA from Roche (Lörrach,
whereas its own secretion seems to be inhibited by somatostatin.22,23
Germany). Free cortisone, free cortisol, tetrahydrocortisol (THF),
Short-term exercise did not lead to changes in ghrelin levels.24 The
αTHF and tetrahydrocortisone (THE) concentrations in 24-h urine
effects of prolonged exercise are unknown.
samples were analysed by RIA.25 11β-HSD-1 activity was calculated by
The aim of this study was to assess the adaptations of the
the ratio (THF + αTHF)/THE, and 11β-HSD-2 activity by the ratio
hypothalamic-pituitary hormonal system to endurance training and
Plasma ghrelin was analysed in all samples from individual sub-
jects in duplicate in the same assay. Immunoreactive total humanplasma ghrelin was measured by RIA (Phoenix Pharmaceuticals,
Materials and methods
Mountain View, CA, USA). Intra- and interassay CV was 5·3% and13·6%, respectively.26
Eight healthy women between 26 and 55 years old and 11 healthy
men between 30 and 66 years old volunteered for this study. The BMIwas 21·6 ± 1·1 kg/m2 and 24·0 ± 1·6 kg/m2 for the female and for the
Statistical calculations were performed with 11·0 (SPSS Inc.,
male athletes, respectively. The VO max was 42·9 ± 2·1 ml/kg
for the female athletes and 48·3 ± 1·8 ml/kg * min for the male
All values are given as mean value and standard error. Paired
athletes. A training log over the whole study period of 12 weeks was
analysis was performed by Wilcoxon test. An alpha-error below 5%
carried out by each runner. All volunteers trained the whole time in
was considered statistically significant.
Berlin at an altitude of about 80 m above sea level and all participantswere requested not to change nutritive behaviour.
All volunteers were screened for serious health problems or use
of any drugs by interview, and an examination was performed by an
In the time before the marathon, there was a significantly higher
experienced sports physician. The experimental protocol was
training level (date 2: 57·5 ± 4·3 km/week, date 4: 20·5 ± 4·0 km/
approved by the institutional review board, and all subjects gave
week, P < 0·05), which is shown by the number of kilometres per
week (Fig. 1). The 42.195 kilometres of the marathon are notincluded in training amounts at date 3 (28·44 ± 5·1 km/week).
The data for ACTH and cortisol are shown in Fig. 2. There was a
significant decrease of ACTH (date 1: 21·5 ± 2·1 ng/l, date 3: 16·7 ±
Metabolic parameters were analysed at five different dates around
1·4 ng / l, date 5: 23·3 ± 3·2 ng/ml, P < 0·05) and cortisol (date 1:
483·5 ± 37·0 nmol/l, date 3: 370·7 ± 25·8 nmol/l, date 5: 446·6 ± 43·3
nmol / l, P < 0·05) 2 days after the marathon, but no differences
were observed in relation to high and low training levels. All ACTH
Date 3: 2 days after real,- Berlin marathon
and cortisol values were in the physiological normal range.
The results of the dexamethasone suppression test showed signi-
ficantly lower levels of cortisol 6 weeks after the marathon with lower
The participants came at 2 days between 8:00 and 9:00 h for blood
training levels (Fig. 3). Significant differences were seen only in date
withdrawal. Before the first day they also collected urine for 24 h. At
5 (date 1: 40·2 ± 4·5 nmol/l, P = 0·008, date 5: 31·6 ± 3·7 nmol/l,
date 1, blood samples were taken for basal values of cortisol, ACTH,
P = 0·037). No differences were found in relation to the marathon
total testosterone, sex hormone binding globulin (SHBG), LH, FSH,
insulin-like growth factor-1 (IGF-1), insulin-like growth factor-
Values for 11β-HSD-1 activity and 11β-HSD-2 activity are shown
binding protein 3 (IGF-BP3), TSH, free thyroxine (fT4), ghrelin and
in Fig. 4. Whereas the activity of the 11β-HSD-2 appeared to
2005 Blackwell Publishing Ltd, Clinical Endocrinology, 63, 530–536 Fig. 1 Kilometres per week between the five examinations (date 1: 6 weeks Fig. 3 Cortisol after 1 mg dexamethasone suppression test. Significant
before marathon, date 2: 10 days before marathon, date 3: 2 days after real,-
changes were marked with brackets. (date 1: 6 weeks before marathon,
Berlin marathon (training amounts did not include the 42.195 kilometres
date 2: 10 days before marathon, date 3: 2 days after real,- Berlin marathon,
of the marathon), date 4: 10 days after marathon, date 5: 6 weeks after
date 4: 10 days after marathon, date 5: 6 weeks after marathon).
marathon). After the marathon there was a significant decrease in running intensity (P < 0·05). Fig. 2 Changes of ACTH and cortisol levels in relation to the marathon. Fig. 4 Activity of HSD 1(circles) and HSD 2 (squares) in 24-h urine.
Significant changes (P < 0·05) in relation to date 3 (2 days after marathon)
Significant changes in relation to date 3 (2 days after marathon) were marked
were marked with * (date 1: 6 weeks before marathon, date 2: 10 days before
with brackets. (date 1: 6 weeks before marathon, date 2: 10 days before
marathon, date 3: 2 days after real,- Berlin marathon, date 4: 10 days after
marathon, date 3: 2 days after real,- Berlin marathon, date 4: 10 days after
marathon, date 5: 6 weeks after marathon).
marathon, date 5: 6 weeks after marathon).
be unaffected, the activity of the 11β-HSD-1 was significantly higher
3: 141·0 ± 8·8 µg/l, P = 0·036) and IGF-BP3 (date 3: 3·7 ± 0·2 mg/l,
2 days after the marathon (date 2: 1·18 ± 0·09, P = 0·013, date 4:
date 5: 4·2 ± 0·2 mg/l, P = 0·045).
Ghrelin levels were basically not different during the study (Fig. 5).
Thyroid-stimulating hormone was significantly lower 6 weeks
Only in relation to 6 weeks after the marathon was there a slight differ-
after the marathon (date 1: 1·13 ± 0·2 mU/l, date 5: 1·03 ± 0·16 mU/l,
ence (date 3: 588·4 ± 51·8 ng/l, date 5: 512·17 ± 41·8 ng/l, P = 0·031). P = 0·024), but free T4 showed no significant changes (date 1: 22·5 ±
Changes in sex hormones were studied only for men, because of
0·8 pmol / l, date 5: 23·3 ± 0·7 pmol/l, P = 0·205). TSH and fT4 values
different cycle times in female volunteers. In male volunteers, no
were in the physiological normal range, but TSH was in a lower normal
changes were observed for LH and FSH (data not shown). However,
range, whereas fT4 was in the high normal range at all time points.
there was a significant increase from all dates to date 5 of the free
IGF-1 and IGF-BP3 were also unaltered in the observed 12 weeks
androgen index (FAI) (date 1: 38·3 ± 3·4, date 2: 41·7 ± 3·3, date 3:
(IGF-1: date 1: 132·1 ± 8·7 µg/l, date 3: 141·2 ± 8·8 µg/l, date 5:
46·0 ± 6·4, date 4: 51·1 ± 3·4, date 5: 58·9 ± 9·5, P < 0·05), which was
147·9 ± 11·5 µg/l, P > 0·05; IGF-BP3: date 1: 4·1 ± 0·2 mg/l, date 3:
calculated by testosterone (date 1: 15·4 ± 1·5 nmol/l, date 2: 16·2 ±
4·0 ± 0·1 mg/l, date 5: 4·3 ± 0·2 mg/l, P > 0·05). Only in men did we
1·3 nmol / l, date 3: 17·3 ± 1·6 nmol/l, date 4: 19·4 ± 1·8 nmol/l, date
find a significant increase of IGF-1 (date 1: 126·7 ± 9·0 µg/l, date
5: 21·8 ± 2·9 nmol/l) and SHBG values (date 1: 40·0 ± 4·5 nmol/l,
2005 Blackwell Publishing Ltd, Clinical Endocrinology, 63, 530–536 Endurance training and pituitary hormonesFig. 5 Plasma samples were taken at all five dates in the morning and were Fig. 7 CRP levels at all dates. CRP at date 3 (2 days after the marathon)
analysed for ghrelin. Significant changes were marked with brackets. (date
was significant higher compared with all other dates. (date 1: 6 weeks before
1: 6 weeks before marathon, date 2: 10 days before marathon, date 3: 2 days
marathon, date 2: 10 days before marathon, date 3: 2 days after real,-
after real,- Berlin marathon, date 4: 10 days after marathon, date 5: 6 weeks
Berlin marathon, date 4: 10 days after marathon, date 5: 6 weeks after
lower basal cortisol levels after endurance training.10,11 In this studyno changes in basal cortisol or ACTH basal levels between a hightraining status (at date 1 or 2) and a low training status (at date 4or 5) were found. However, there was a trend to an up-regulationof the HPA system, because the dexamethasone suppression test,which is an indicator for the sensitivity of the HPA system, showedsignificant lower levels of cortisol after 6 weeks of lower traininglevels in relation to high training levels. In combination with theresults of unaltered basal cortisol levels, it seems that the sensitivityof the HPA axis is changed. At a training status with an elevated train-ing amount, the HPA axis is more resistant to dexamethasone thanin a moderate training status with only a few kilometres per week. Similar results were found in a cross-sectional study performed inendurance-trained and untrained men, although a dexamethasone-CRH test was applied in this study.9 It is also known that the tissue
Fig. 6 For all male volunteers, free androgen index was calculated by
sensitivity to glucocorticoids in endurance-trained men is decreased.27
testosterone × 100/SHBG. FAI at date 5 (6 weeks after marathon) was
Changes in sensitivity to glucocorticoids may explain the discrep-
significantly higher compared with all other dates. (date 1: 6 weeks before
ancy between repeated and prolonged exercise-induced HPA axis
marathon, date 2: 10 days before marathon, date 3: 2 days after real,- Berlin
activation and the lack of metabolic consequences of such increased
marathon, date 4: 10 days after marathon, date 5: 6 weeks after marathon).
We found reduced plasma levels of cortisol and ACTH 2 days after
date 2: 39·1 ± 4·5 nmol/l, date 3: 37·4 ± 4·3 nmol/l, date 4: 37·9 ± 4·4
the marathon. This was probably an acute effect of the marathon and
nmol / l, date 5: 37·4 ± 4·3 nmol/l) (Fig. 6).
not related to training changes. The results suggest that the extreme
We also aimed to detect general inflammation or possible infec-
physical stress of the marathon7 causes a short-term exhaustion of
tions. Therefore, CRP was measured at all time points (Fig. 7). There
was a significant increase of CRP in the physiological normal range
As a result of the exhaustion of the ACTH-cortisol axis after the
2 days after the marathon (date 3: 5·4 ± 0·6 mg/l, P < 0·005).
marathon, the tissues expressing 11β-HSD-1 may regulate cortisolmetabolism against the low-circulating cortisol levels. Indeed, theactivity of the 11β-HSD-1 was increased 2 days after the marathon,
Discussion
whereas the activity of the 11β-HSD-2 was slightly reduced. Thus,
In this study, the effects of intensive endurance training on the
the impaired sensitivity of the systemic HPA axis appears to be coun-
hypothalamic-pituitary axis were examined.
terbalanced by increased availability of cortisol by increased local
Previous reports suggested that endurance training is associated
activation from cortisone to the more active cortisol. Similar results
with subclinical hypercortisolism,3,8 whereas others reported even
are found in the circadian rhythm of the 11β-HSD activity. Low
2005 Blackwell Publishing Ltd, Clinical Endocrinology, 63, 530–536
cortisol values at midnight are maybe compensated by a higher activ-
androgen index (FAI) was significantly higher after reduction of
endurance exercise. Changes in testosterone values through physical
Generally, CRP levels were relatively low in the investigated indi-
activity depend of the kind of training. Lower testosterone levels have
viduals, which was probably to the result of the ongoing endurance
been shown in endurance-trained men compared with sedentary
training.29,30 The extreme physical stress during the marathon caused
controls,41,42 whereas resistance-trained persons seem to have higher
a substantial increase of CRP values as detected 2 days after the race.
basal testosterone levels.43,44 Thereby endurance- and resistant-
Although elevation of CRP usually indicates an ongoing systemic
trained persons had lower testosterone levels than sedentary control
inflammatory reaction31 we found no elevated cortisol levels like
subjects.45 It is also known that high cortisol levels, e.g. in patients
that found in ill persons.32 Interestingly, there were no differences
with Cushing’s syndrome, lead to a suppression of the gonadal axis
between high and low training levels. However, the time periods with the
with lowered values for testosterone.46 The present study supports
respective training levels may have been too short to see any changes.
the previously found results. Thereby this lowered testosterone level
Although there was a trend towards higher ghrelin levels directly
does not seem to induce pathological reactions like decreased bone
after the marathon, no dramatic differences were seen. This result is
density47 or decreased physical fitness.48 Furthermore, testosterone
in line with a recent publication showing that acute exercise does not
concentrations have been shown to increase after an acute bout
change circulating ghrelin levels in humans.24 The slightly increased
of resistance or endurance exercise.49,50 In response to prolonged
ghrelin levels 2 days after the marathon could be still a sign of a negative
endurance exercise (e.g. running a marathon), testosterone levels
energy balance after the marathon, which is known to induce higher
will typically decline.51,52 In this study, the time after the marathon
(2 days) was probably too long to see any acute changes resulting
The changes of IGF-1 and IGF-BP3 were not significant, but there
was a trend towards increasing levels of IGF-1 and IGF-BP3 during
In summary, this study has shown acute and prolonged changes
lower training levels. However, these findings are only significant in
in pituitary hormone axes as a result of marathon training and run-
men, but not in women. One year of endurance training above the
ning a marathon. In particular, the adaptations in the HPA system
lactate threshold has been shown to cause an increase in basal 24-h
showed decreased levels of cortisol after the marathon and decreased
pulsatile GH release.35 Interestingly, subjects training below the lac-
sensitivity of glucocorticoid-regulation during a stage of high training
tate threshold did not show any change in the GH release, indicating
intensity. Furthermore, cortisol metabolism by the 11β-HSD system is
that training intensity may be important in regulating the GH axis.
altered after the marathon. Concerning the acute down-regulation
Therefore, the study group was perhaps too inhomogeneous to see any
of ACTH and cortisol after the marathon, further studies with
differences in the hypothalamic-pituitary-growth hormone axis.
dynamic testing (CRH test, metyrapone test) would be interesting.
We found no acute effect 2 days after the marathon, whereas otherstudies have shown that IGF-1 and IGF-BP3 increase after acute
Acknowledgements
exercise.36,37 However, the duration of the postexercise elevation ofIGF-1 and IGF-BP3 might be short and we thus might have missed
We thank Petra Exner and Katrin Sprengel for excellent technical
a peak directly after the marathon. Additionally in our study, all
assistance. JS was supported by the BMBF (0313036B), the Eli-Lilly
investigated individuals had a relatively high training status and the
International Foundation (ELIF21001) and the German Diabetes
IGF-1/IGF-BP3 levels might have reached a relative plateau, explain-
Association (DDG021006). We thank also the real,- Berlin marathon
ing that there was no additional increase after the acute exercise.
The thyroidal axis was also altered by marathon training. TSH,
during the time of lower training exercise, was significantly lower
References
than during intensive training, whereas fT4 was also higher after a
1 Albright, A., Franz, M., Hornsby, G., Kriska, A., Marrero, D., Ullrich, I.
phase of lower training exercise, but these changes were not significant.
& Verity, L.S. (2000) American College of Sports Medicine position
Similar results with increased levels of TSH and slightly reduced
stand. Exercise and type 2 diabetes. Medicine & Science in Sports and
levels of T3 after 3 months were found in obese women.38 Acute
Exercise, 32, 1345 – 1360.
exercise does not induce any changes in the thyroidal axis.39 In
2 Bunt, J.C. (1986) Hormonal alterations due to exercise. Sports
accordance with these findings, there was no acute effect 2 days after
Medicine, 3, 331 –345.
the marathon. The data concerning thyroidal hormones and exercise
3 Luger, A., Deuster, P.A., Kyle, S.B., Gallucci, W.T., Montgomery, L.C.,
are very controversial. Regarding the thyroid hormone response to
Gold, P.W., Loriaux, D.L. & Chrousos, G.P. (1987) Acute hypothalamic-
endurance exercise in humans, there exist studies with increases and
pituitary-adrenal responses to the stress of treadmill exercise.
decreases in TSH levels.40 A possible cause of these differences
Physiologic adaptations to physical training. New England Journal of
between studies and individuals might be variations in plasma
Medicine, 316, 1309 –1315.
4 Hakkinen, K. & Pakarinen, A. (1995) Acute hormonal responses to
volume after exercise, i.e. haemoconcentration or haemodilution.
heavy resistance exercise in men and women at different ages. Inter-
Therefore, the effects of endurance training on thyroid function still
national Journal of Sports Medicine, 16, 507 –513.
5 Deuster, P.A., Chrousos, G.P., Luger, A., DeBolt, J.E., Bernier, L.L.,
In male participants, the hypothalamic-pituitary-gonadal axis
Trostmann, U.H., Kyle, S.B., Montgomery, L.C. & Loriaux, D.L.
was altered in this study. LH and FSH did not show any significant
(1989) Hormonal and metabolic responses of untrained, moderately
variances during this study, whereas LH slightly increased and FSH
trained, and highly trained men to three exercise intensities.
decreased during the period of lower training intensity. The free
Metabolism, 38, 141–148.
2005 Blackwell Publishing Ltd, Clinical Endocrinology, 63, 530–536 Endurance training and pituitary hormones
6 McCall, G.E., Byrnes, W.C., Fleck, S.J., Dickinson, A. & Kraemer, W.J.
and interactions with hexarelin, a nonnatural peptidyl GHS, and
(1999) Acute and chronic hormonal responses to resistance training
GH-releasing hormone. Journal of Clinical Endocrinology and Metab-
designed to promote muscle hypertrophy. Canadian Journal ofolism, 86, 1169 –1174. Applied Physiology, 24, 96 –107.
22 Broglio, F., Koetsveld, P.P., Benso, A., Gottero, C., Prodam, F.,
7 Fournier, P.E., Stalder, J., Mermillod, B. & Chantraine, A. (1997)
Papotti, M., Muccioli, G., Gauna, C., Hofland, L., Deghenghi, R.,
Effects of a 110 kilometers ultra-marathon race on plasma hormone
Arvat, E., Van Der Lely, A.J. & Ghigo, E. (2002) Ghrelin secretion is
levels. International Journal of Sports Medicine, 18, 252 –256.
inhibited by either somatostatin or cortistatin in humans. Journal of
8 Villanueva, A.L., Schlosser, C., Hopper, B., Liu, J.H., Hoffman, D.I. Clinical Endocrinology and Metabolism, 87, 4829 – 4832.
& Rebar, R.W. (1986) Increased cortisol production in women run-
23 Schaller, G., Schmidt, A., Pleiner, J., Woloszczuk, W., Wolzt, M. &
ners. Journal of Clinical Endocrinology and Metabolism, 63, 133 –136.
Luger, A. (2003) Plasma ghrelin concentrations are not regulated by
9 Duclos, M., Corcuff, J.B., Pehourcq, F. & Tabarin, A. (2001) Decreased
glucose or insulin: a double-blind, placebo-controlled crossover
pituitary sensitivity to glucocorticoids in endurance-trained men.
clamp study. Diabetes, 52, 16 – 20. European Journal of Endocrinology, 144, 363 – 368.
24 Kraemer, R.R., Durand, R.J., Acevedo, E.O., Johnson, L.G., Kraemer, G.R.,
10 Uusitalo, A.L., Huttunen, P., Hanin, Y., Uusitalo, A.J. & Rusko, H.K.
Hebert, E.P. & Castracane, V.D. (2004) Rigorous running increases
(1998) Hormonal responses to endurance training and overtraining
growth hormone and insulin-like growth factor-I without altering
in female athletes. Clinical Journal of Sports Medicine, 8, 178 –186.
ghrelin. Experimental Biology and Medicine (Maywood), 229, 240 –
11 Lucia, A., Diaz, B., Hoyos, J., Fernandez, C., Villa, G., Bandres, F. &
Chicharro, J.L. (2001) Hormone levels of world-class cyclists during
25 Maser-Gluth, C., Reincke, M., Allolio, B. & Schulze, E. (2000) Metab-
the Tour of Spain stage race. British Journal of Sports Medicine, 35,
olism of glucocorticoids and mineralocorticoids in patients with
adrenal incidentalomas. European Journal of Clinical Investigations,
12 Maestu, J., Jurimae, J. & Jurimae, T. (2003) Hormonal reactions
30 (Suppl. 3), 83 – 86.
during heavy training stress and following tapering in highly trained
26 Otto, B., Tschop, M., Heldwein, W., Pfeiffer, A.F. & Diederich, S.
male rowers. Hormone and Metabolic Research, 35, 109 –113.
(2004) Endogenous and exogenous glucocorticoids decrease plasma
13 Quinkler, M., Troeger, H., Eigendorff, E., Maser-Gluth, C., Stiglic, A.,
ghrelin in humans. European Journal of Endocrinology, 151, 113 –117.
Oelkers, W., Bahr, V. & Diederich, S. (2003) Enhanced 11beta-
27 Duclos, M., Gouarne, C. & Bonnemaison, D. (2003) Acute and
hydroxysteroid dehydrogenase type 1 activity in stress adaptation in
chronic effects of exercise on tissue sensitivity to glucocorticoids.
the guinea pig. Journal of Endocrinology, 176, 185 –192. Journal of Applied Physiology, 94, 869 – 875.
14 Quinkler, M. & Stewart, P.M. (2003) Hypertension and the cortisol-
28 Quinkler, M., Oelkers, W. & Diederich, S. (2001) Clinical implica-
cortisone shuttle. Journal of Clinical Endocrinology and Metabolism,
tions of glucocorticoid metabolism by 11beta-hydroxysteroid
88, 2384 –2392.
dehydrogenases in target tissues. European Journal of Endocrinology,
15 Koistinen, H., Koistinen, R., Selenius, L., Ylikorkala, Q. & Seppala, M. 144, 87 – 97.
(1996) Effect of marathon run on serum IGF-I and IGF-binding pro-
29 Mattusch, F., Dufaux, B., Heine, O., Mertens, I. & Rost, R. (2000)
tein 1 and 3 levels. Journal of Applied Physiology, 80, 760 –764.
Reduction of the plasma concentration of C-reactive protein follow-
16 Ehrnborg, C., Lange, K.H., Dall, R., Christiansen, J.S., Lundberg, P.A.,
ing nine months of endurance training. International Journal of
Baxter, R.C., Boroujerdi, M.A., Bengtsson, B.A., Healey, M.L.,
Sports Medicine, 21, 21 – 24.
Pentecost, C., Longobardi, S., Napoli, R. & Rosen, T. (2003) The
30 Tomaszewski, M., Charchar, F.J., Przybycin, M., Crawford, L.,
growth hormone/insulin-like growth factor-I axis hormones and
Wallace, A.M., Gosek, K., Lowe, G.D., Zukowska-Szczechowska, E.,
bone markers in elite athletes in response to a maximum exercise test.
Grzeszczak, W., Sattar, N. & Dominiczak, A.F. (2003) Strikingly low
Journal of Clinical Endocrinology and Metabolism, 88, 394 – 401.
circulating CRP concentrations in ultramarathon runners independ-
17 Deuschle, M., Blum, W.F., Frystyk, J., Orskov, H., Schweiger, U.,
ent of markers of adiposity: how low can you go? Arteriosclerosis,
Weber, B., Korner, A., Gotthardt, U., Schmider, J., Standhardt, H. &
Thrombosis and Vascular Biology, 23, 1640 –1644.
Heuser, I. (1998) Endurance training and its effect upon the activity
31 Frey, W., Wassmer, P., Frey-Rindova, P., Braun, D., Schwarz, F.,
of the GH-IGFs system in the elderly. International Journal of Sports
Arnold, M., Piguet, A. & Villiger, B. (1994) Muscle aches and bio-
Medicine, 19, 250 –254.
chemical changes following a ultra-marathon in the cold modification
18 Kojima, M., Hosoda, H., Date, Y., Nakazato, M., Matsuo, H. &
by diclofenac. Schweizerische Zeitschrift Fur Medizin Und Traumato-
Kangawa, K. (1999) Ghrelin is a growth-hormone-releasing acylated
peptide from stomach. Nature, 402, 656 – 660.
32 Boss, B. & Neeck, G. (2000) Correlation of IL-6 with the classical
19 Takaya, K., Ariyasu, H., Kanamoto, N., Iwakura, H., Yoshimoto, A.,
humoral disease activity parameters ESR and CRP and with serum
Harada, M., Mori, K., Komatsu, Y., Usui, T., Shimatsu, A., Ogawa, Y.,
cortisol, reflecting the activity of the HPA axis in active rheumatoid
Hosoda, K., Akamizu, T., Kojima, M., Kangawa, K. & Nakao, K.
arthritis. Zeitschrift für Rheumatologie, 59, II/62 –II/64.
(2000) Ghrelin strongly stimulates growth hormone release in humans.
33 Toshinai, K., Mondal, M.S., Nakazato, M., Date, Y., Murakami, N.,
Journal of Clinical Endocrinology and Metabolism, 85, 4908 – 4911.
Kojima, M., Kangawa, K. & Matsukura, S. (2001) Upregulation of
20 Mozid, A.M., Tringali, G., Forsling, M.L., Hendricks, M.S., Ajodha, S.,
Ghrelin expression in the stomach upon fasting, insulin-induced
Edwards, R., Navarra, P., Grossman, A.B. & Korbonits, M. (2003)
hypoglycemia, and leptin administration. Biochemistry and Biophysics
Ghrelin is released from rat hypothalamic explants and stimulates
Research Communications, 281, 1220 –1225.
corticotrophin-releasing hormone and arginine-vasopressin.
34 Muccioli, G., Tschop, M., Papotti, M., Deghenghi, R., Heiman, M. Hormone and Metabolism Research, 35, 455 – 459.
& Ghigo, E. (2002) Neuroendocrine and peripheral activities of ghre-
21 Arvat, E., Di Maccario, M.V.L., Broglio, F., Benso, A., Gottero, C.,
lin: implications in metabolism and obesity. European Journal of
Papotti, M., Muccioli, G., Dieguez, C., Casanueva, F.F., Deghenghi, R.,
Pharmacology, 440, 235 – 254.
Camanni, F. & Ghigo, E. (2001) Endocrine activities of ghrelin, a nat-
35 Weltman, A., Weltman, J.Y., Schurrer, R., Evans, W.S., Veldhuis, J.D.
ural growth hormone secretagogue (GHS), in humans: comparison
& Rogol, A.D. (1992) Endurance training amplifies the pulsatile
2005 Blackwell Publishing Ltd, Clinical Endocrinology, 63, 530–536
release of growth hormone: effects of training intensity. Journal of
Putukian, M. & Evans, W.J. (1999) Effects of heavy resistance training
Applied Physiology, 72, 2188 –2196.
on hormonal response patterns in younger vs. older men. Journal of
36 Bang, P., Brandt, J., Degerblad, M., Enberg, G., Kaijser, L., Thoren, M. Applied Physiology, 87, 982 –992.
& Hall, K. (1990) Exercise-induced changes in insulin-like growth
45 Arce, J.C., De Souza, M.J., Pescatello, L.S. & Luciano, A.A. (1993)
factors and their low molecular weight binding protein in healthy
Subclinical alterations in hormone and semen profile in athletes.
subjects and patients with growth hormone deficiency. EuropeanFertility and Sterility, 59, 398 – 404. Journal of Clinical Investigations, 20, 285 – 292.
46 Smals, A.G., Kloppenborg, P.W. & Benraad, T.J. (1977) Plasma
37 Cappon, J., Brasel, J.A., Mohan, S. & Cooper, D.M. (1994) Effect of
testosterone profiles in Cushing’s syndrome. Journal of Clinical
brief exercise on circulating insulin-like growth factor I. Journal ofEndocrinology and Metabolism, 45, 240 –245. Applied Physiology, 76, 2490 – 2496.
47 Maimoun, L., Lumbroso, S., Manetta, J., Paris, F., Leroux, J.L. &
38 Krotkiewski, M., Sjostrom, L., Sullivan, L., Lundberg, P.A., Lindstedt, G.,
Sultan, C. (2003) Testosterone is significantly reduced in endurance
Wetterqvist, H. & Bjorntorp, P. (1984) The effect of acute and chronic
athletes without impact on bone mineral density. Hormone Research,
exercise on thyroid hormones in obesity. Acta Medica Scandinavia,
59, 285 – 292. 216, 269 –275.
48 Urhausen, A., Kullmer, T. & Kindermann, W. (1987) A 7-week
39 Huang, W.S., Yu, M.D., Lee, M.S., Cheng, C.Y., Yang, S.P., Chin, H.M.
follow-up study of the behaviour of testosterone and cortisol during
& Wu, S.Y. (2004) Effect of treadmill exercise on circulating thyroid
the competition period in rowers. European Journal of Applied
hormone measurements. Medical Principles and Practices, 13, 15 – 19. Physiology and Occupational Physiology, 56, 528 – 533.
40 Chicharro, J.L., Hoyos, J., Bandres, F., Terrados, N., Fernandez, B. &
49 Kraemer, R.R., Kilgore, J.L., Kraemer, G.R. & Castracane, V.D. (1992)
Lucia, A. (2001) Thyroid hormone levels during a 3-week profes-
Growth hormone, IGF-I, and testosterone responses to resistive
sional road cycling competition. Hormone Research, 56, 159 –164.
exercise. Medicine & Science in Sports & Exercise, 24, 1346 –1352.
41 Hackney, A.C., Sinning, W.E. & Bruot, B.C. (1988) Reproductive
50 McMurray, R.G., Eubank, T.K. & Hackney, A.C. (1995) Nocturnal
hormonal profiles of endurance-trained and untrained males.
hormonal responses to resistance exercise. European Journal ofMedicine & Science in Sports & Exercise, 20, 60 – 65. Applied Physiology and Occupational Physiology, 72, 121 –126.
42 Wheeler, G.D., Wall, S.R., Belcastro, A.N. & Cumming, D.C. (1984)
51 Dressendorfer, R.H. & Wade, C.E. (1991) Effects of a 15-d race on
Reduced serum testosterone and prolactin levels in male distance
plasma steroid levels and leg muscle fitness in runners. Medicine &
runners. Journal of the American Medical Association, 252, 514 –516. Science in Sports & Exercise, 23, 954 – 958.
43 Hakkinen, K., Pakarinen, A., Alen, M., Kauhanen, H. & Komi, P.V.
52 Keizer, H., Janssen, G.M., Menheere, P. & Kranenburg, G. (1989)
(1988) Neuromuscular and hormonal adaptations in athletes to strength
Changes in basal plasma testosterone, cortisol, and dehydroepian-
training in 2 years. Journal of Applied Physiology, 65, 2406 – 2412.
drosterone sulfate in previously untrained males and females pre-
44 Kraemer, W.J., Hakkinen, K., Newton, R.U., Nindl, B.C., Volek, J.S.,
paring for a marathon. International Journal of Sports Medicine, 10,
McCormick, M., Gotshalk, L.A., Gordon, S.E., Fleck, S.J., Campbell, W.W.,
2005 Blackwell Publishing Ltd, Clinical Endocrinology, 63, 530–536
New Zealand white rabbits were treated with Retin-A Micro (tretinoin gel) microsphere, 0.1%, at doses of 0.2, 0.5, and 1.0 mg/kg/day, administered topical y for 24 hours a day while wearing Elizabethan col ars to prevent ingestion of the drug. There appeared to be increased incidences of certain alterations, including domed head and hydrocephaly, typical of retinoid-induced fetal malformations
2012 Express Scripts National Preferred Preventive Drug List Prescription Drugs: You Make the Choices, We Make it Easy Preventive Prescription Drugs: A Good Choice Prescription drugs that can help keep you from developing a health condition are cal ed preventive prescription drugs. They can help you maintain your quality of life and avoid expensive treatment, helping to reduce your ov
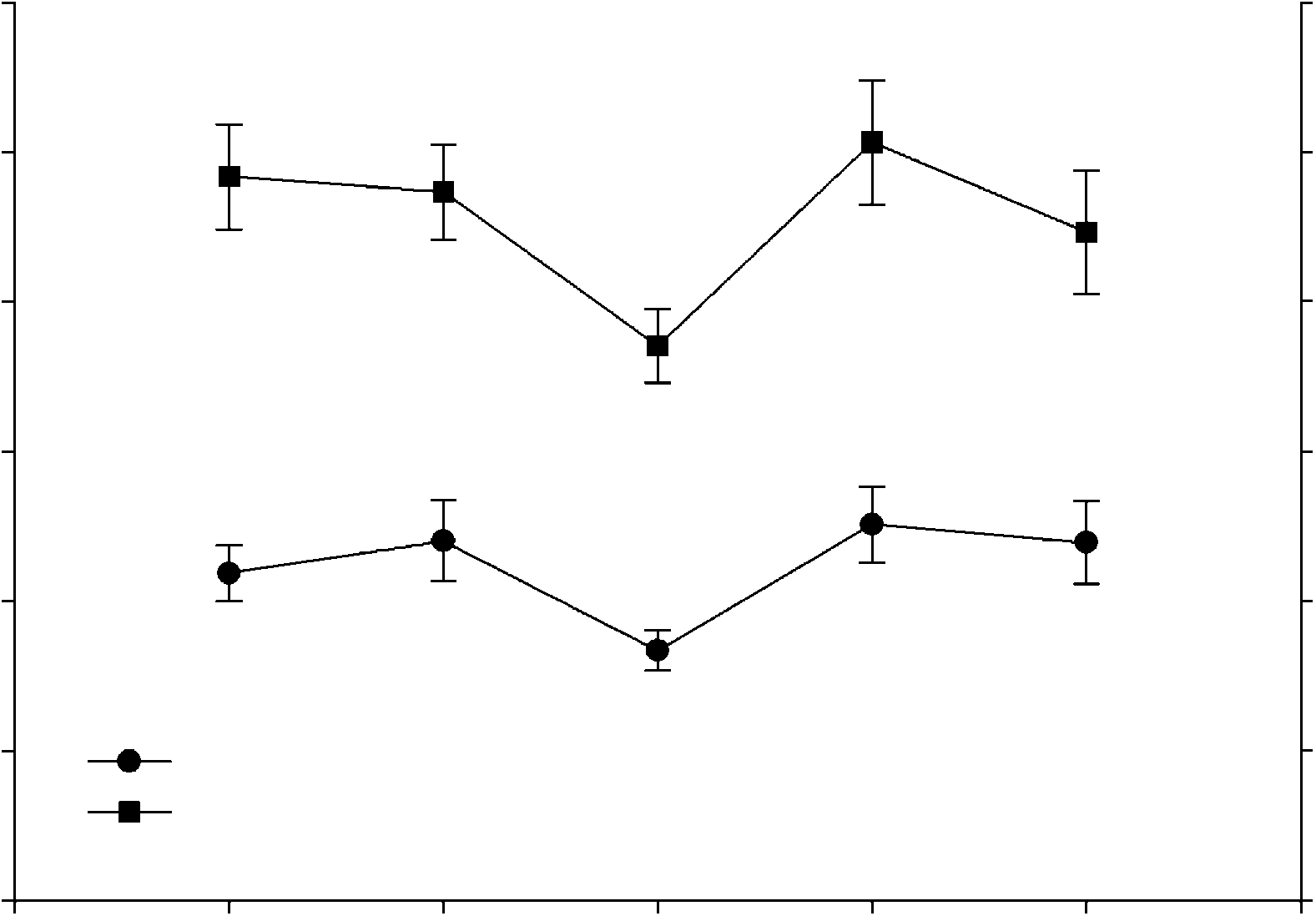 Fig. 1 Kilometres per week between the five examinations (date 1: 6 weeks
Fig. 1 Kilometres per week between the five examinations (date 1: 6 weeks