intensetimes issue 12. Spring 2011 Aspects of severe heart failure
A wide-ranging debate about many aspects of severe heart failure opened with a review by Professor Anthony McLean (Sydney, NSW, Australia) of evidence for the premise that heart failure in most if not all of its many manifestations is an inflammatory disorder – or at least a condition in which signs usually associated with inflammation are often encountered. Professor McLean conceded that there are some anomalies that do not fit easy with the idea of heart failure as fundamentally an inflammatory condition but nevertheless felt that inflammation needs to be taken more seriously as an aspect of heart failure, both as a mechanism and as a potential target for intervention.
Following on from Professor McLean, Professor Karl Werdan (Halle, Germany) set a precedent for other speakers by modifying the official title of his talk. In this case the alteration was the small but significant addition of a question mark to the phrase “Sepsis is the main cause of death.” The message of this amendment seemed clear: sepsis may be a major cause of death, but this is unlikely to be universally the case.
One strand of the evidence connecting heart failure with sepsis may be traced to the endotoxaemia theory of Niebauer and colleagues (Lancet 1999;353:1838–42); the essence this theory was that mesenteric congestion created circumstances in which endotoxaemia might develop. (Inflammation was also thought to be an essential feature of this cascade.) Reports such as that of O‟Malley and colleagues (Br J Anaesth 2004;92:131–3), who described an association between high intra-operative plasma levels of endotoxin and adverse postoperative outcome lent support to the view that endotoxaemia might be caused by gut hypoperfusion during surgery and was associated with postoperative organ dysfunction.
Professor Werdan identified cardiogenic shock (CS) as the aspect of heart failure most likely to be associated with sepsis. He commented that there are two distinct presentations of CS: one surprisingly benign and often following a relatively uneventful course to recovery; the other a crisis of survival associated with MOF. Drawing on experience in the SHOCK study (Kohsaka S et al. Am J Cardiol 2007;99:802–4), Professor Werdan said that evidence of systemic inflammatory response syndrome (SIRS) suggestive of sepsis is encountered in some 15% of patients with CS. Noting that a collapse in SVR is the primary haemodynamic feature of sepsis in CS, he suggested that both systemic inflammation and sepsis may exert their deleterious effects by preventing compensatory vasoconstriction.a
intensetimes issue 12. Spring 2011 Measuring contractility Regardless of whatever other factors may be operating it is hard not to regard severe heart failure as being at some level a problem of inadequate cardiac contractility. This in turn places a premium on being able to measure contractility. However, according to Dr Sabino Scolletta (Siena, Italy) the gold standard of the physiology laboratory – measuring the maximum velocity of contraction of an isolated myocardial fibre not subject to load – clearly is not applicable in the clinic. All the methods that may be used clinically have their limitations and at present no single measurement meets the criteria for a fully satisfactory measure of contractility. Indeed, it may be argued (and Dr Scolletta did) that it is infeasible that a single number can adequately characterize the complex geometric and volumetric functions of the left ventricle: multiple parallel measures are needed to give a realistic and relevant estimate. Measures in clinical use for the estimation of myocardial contractility currently include:
The first of these measures suffers from the limitation that it is influenced by preload and may not therefore faithfully reflect contractility (for which stroke volume is a surrogate).
There is a wide range of ejection-phase indices, most of which can be obtained via echocardiography, but overwhelmingly the one first called upon by clinicians wanting some simple indicator of contractility is left ventricular ejection fraction (LVEF). This also is subject to influence by cardiac loading; moreover, and partly because of the influence of preload, LVEF does not in fact reflect changes in contractility in a failing heart, especially during the early phases of failure when compensatory mechanisms are functional. Nevertheless, in the absence of anything better (or more easily appreciated), LVEF seems likely to remain a staple of clinical assessment for some time (see McGowan JH, Cleland JG. Am Heart J 2003;146:388–97 & Schiller NB. idem 380–2, for some perspectives on this matter).
Transoesophageal echocardiography with thermodilution has been used to derive the cardiac function index (CFI) and the global ejection fraction (GEF) from the left ventricular fractional area of change (LVFAC) in mechanically ventilated ICU patients (see Panel on page 8 for definitions) (Combes A et al. Intensive Care Med 2004;30:1377–83. CFI >4 and GEF >18% were both identified as indicators of good intensetimes issue 12. Spring 2011
ventricular systolic function. However, as the derivation of GEF includes the volume of the right ventricle, dilatation of the right ventricle can lead to underestimation of left ventricular contractility.
Among isovolumic-phase indices, the rate of development of pressure (dP/dT) measured by continuous wave Doppler echocardiography has attracted attention, with indications that it may be predictive of survival in congestive heart failure (Kolias TJ et al. J Am Coll Cardiol 2000;36:1594–9), but the method suffers from certain limitations including a degree of preload-dependency. In addition, it can be compromised by ventricular dys-synchrony and the presence of regurgitant jets. Moreover, this invasive technique is not suited to routine bedside use.
Optimal ventricular function requires optimized ventricular-arterial coupling, noted Dr Scolletta. This provides another way to evaluate ventricular contractility. The principles of this method are illustrated in Figure A (see page 9 of this file). Two of the three parameters needed to calculate the ratio of arterial elastance (Ea) and end-systolic ventricular elastance (Ees) may be obtained by echocardiography; however, the third, end-systolic pressure requires an invasive procedure. A low Ea/Ees ratio signifies good ventricular-arterial coupling and vice versa, and can be predictive of medium-term survival post-MI (Antonini-Canterin F J Am Soc Echocardiogr 2009;22:1239–45).
Dr Alexandre Mebazaa (Paris, France) used two presentations to pass on some key messages about drug therapy in severe heart failure.
The first message concerned the use of beta-blockers and was simple.
Patients on beta-blockers at admission should be maintained on beta-blockers if
Patients not on beta-blockers at admission or removed from beta-blockers after
admission should be put onto a beta-blocker as early as possible and certainly before discharge (see Jondeau G et al. Eur Heart J 2009;30:2186–92; Mebazaa A et al. Eur J Heart Fail 2009;11:304–11 and Böhm M et al. Crit Care Med 2011;Jan 28 [Epub ahead of print]) as a examples of the data that led Dr Mebazaa to these conclusions).
The same principles apply to patients admitted with acute respiratory failure whether of cardiac or non-cardiac origin (see Noveanu M et al. Crit Care 2010;14:R198 for more on the Basel-II-ICU study, results of which underpinned this recommendation).
intensetimes issue 12. Spring 2011
Next for Dr Mebazaa‟s attention were the findings of the ALARM-HF study. This retrospective exercise examined inhospital mortality in 4953 patients with acute heart failure admitted to the ICU of cardiac care units and related outcomes to the use of parenteral drugs (Mebazaa A et al. Intensive Care Med 2011;37:290–301). The technique of propensity scoring was used to identify groups of patients who differed by treatment but had the same (multivariate) distribution of covariates. (Propensity scoring is a relatively new concept in ICU medicine and not all the previous exercises were methodologically robust: see Gayat E et al. Intensive Care Med 2010;36:1993–2003 for a review of limitations in earlier exercises of this sort in ICU medicine.)
Use of all four of the mainstream catecholamines – adrenaline, noradrenaline, dopamine and dobutamine – was associated with materially worsened risk of dying within 30 days of admission, reported Dr Mebazaa. By contrast, propensity- matched pairs (n=1007) revealed a lower mortality with the use of diuretics plus vasodilators compared with diuretics alone (7.8% vs 11.0%; p=0.016).
Based on these data, Dr Mebazaa re-iterated the advice that management of acute heart failure should give greater emphasis to the use of drugs with vasodilator properties whereas use of catecholamines should be curtailed. He considered that catecholamines might have value in the 10–15% of patients with CS but that otherwise may be expected to do more harm than good.
High-dose insulin – really high dose
Professor John J Marini (Minneapolis/St Paul, MN, USA) had been invited to address the topic „Insulin can help‟ in the context of severe heart failure but he followed the trend for amending this title to emphasize the significance of dosage. Professor Marini stressed that his research has involved truly heroic doses of insulin: for example, far larger than those evaluated in trials of glucose–insulin–potassium therapy (see, e.g., Ranasinghe AM et al. Circulation 2006;114(1 Suppl):I245–50). In addition, he emphasized that he thought insulin was unlikely to have general therapeutic applications in the setting of heart failure, but that it might have uses in specific situations.
Underpinning Professor Marini‟s research is the belief (backed by observations) that insulin continues to exert potentially positive effects on the cardiovascular system at doses far in excess of what is needed for glucose homoeostasis. (These effects comprise enhanced inotropism and vasodilatation.) This may (or may not) be relevant to chronic heart failure but, provided the effects of these massive doses on glucose and
intensetimes issue 12. Spring 2011
potassium are offset, the cardiovascular effects may be useful in situations such as post-surgery cardiac dysfunction and, most especially, overdosage with cardiotoxic agents, including beta-blockers, calcium-channel blockers (CCBs) and bupivacaine (see Kim JT et al. Anesth Analg 2004;99:728–33.)
Marini and coworkers have already registered some remarkable preclinical results with high-dose insulin (HDI) (see, e.g., Holger JS et al. Acad Emerg Med 2010;17:429–35) and have evidence from still unpublished experiments that euglycaemic HDI prevents propranolol-induced death by promoting a recovery of cardiac output. They have also started to generate clinical data, including a case-report (Holger JS et al. Clin Toxicol (Phila) 2009;47:303–7) of a 65-year-old woman who presented in respiratory arrest and severe myocardial toxicity due to an overdose of amitriptyline and citalopram. (The patient had also consumed several other drugs.) After resuscitation from cardiac arrest and with a still-deteriorating clinical condition, the patient received HDI started at 1 U/kg/h and titrated to 6 U/kg/h (600 U/h) while simultaneously being weaned off noradrenaline and vasopressin. HDI was associated with a near-immediate improvement in urinary flow, metabolic acidosis and skin temperature, while cardiac output nearly tripled (from 3.2 to 11 L/min). HDI was tapered off after 2 days and the patient made a very good recovery.
Professor Marini and his colleagues have now amassed 12 cases of patients with drug-induced cardiotoxicity. These patients received euglycaemic HDI at up to 21 U/kg/h for up to 25.5 h (and glucose for a further average of 21 h).c Eleven of the 12 patients survived this treatment, which was considered to be well tolerated.
Euglycaemic HDI is still at a very early stage of evolution. Some of the things that are already known are that it is necessary to monitor cardiac output continuously, to have central monitoring of glucose and potassium, and to titrate decrementally to effect. Still to be established are optimum dosing and ideal timing. However, Professor Marini saw a useful future for this intervention. He pointed out that as the cellular effects of insulin – and hence the therapeutic effects of euglycaemic HDI – span a range of cardiotoxic mechanisms, HDI may be a real contender for first-line use in cases of cardiotoxicity arising from mixed-drug overdoses of uncertain composition. In this context he suggested that there may also be scope for combining HDI with other agents: for example, a combination of HDI with levosimendan would seem logical in cases of CCB toxicity. intensetimes issue 12. Spring 2011 Mechanical options When drug options are exhausted, some patients may be candidates for mechanical-assist devices. In theory, there are various sorts to choose from, but in practice the choice for the „crash and burn‟ patient with an acute crisis presentation comes down to one – extracorporeal membrane oxygenation (ECMO). Professor Alain Combes (Paris, France) made the case for ECMO simply and convincingly under the following headings:
1. It is relatively easy to implement 2. It works pretty well 3. It works better (or at least as well as) other mechanical-assist options 4. It costs a lot less than other mechanical-assist options.
In the first of these four categories, Professor Combes noted that peripheral-access ECMO can be initiated quickly, with minimal surgical procedures, and that ECMO provides simultaneous cardiac and pulmonary assistance, and high and stable output flow.
As to „working pretty well‟ Sheu et al. have reported long-term (30-day) survival rates in the region of 60% in a series of patients with profound or refractory cardiogenic shock (Crit Care Med 2010;38:1810–17). Is this good? It certainly is better than the rates that previously prevailed in such patients (Combes et al. Crit Care Med 2008;36:1404–11). ECMO was also associated with superior short-term and long-term survival benefit versus conventional cardiopulmonary resuscitation in patients with in-hospital cardiac arrest of cardiac origin in the study by Chen and colleagues (Lancet 2008;372:554–61).
Separately Pages et al. have demonstrated (in a very small patient group: n=11) that ECMO was comparable to a biventricular-assist device as a bridge to recovery for patients with fulminant cardiogenic shock associated with myocarditis, and produced more favourable profiles of biochemistry indices such as bilirubin and creatinine. ECMO has its limitations of course, including the need for recipients of femoral ECMO to remain supine (plus a time limit of 2–3 weeks on delivering ECMO via femoral access). It is, nevertheless, in Professor Combes view, far and away the best option for the acute phase; its only significant rival in that application is the miniature intra-aortic pump (Impella®, Abiomed), which Professor Combes regarded as being limited in several respects (including reliability) if used beyond a few hours and a potential for inducing haemolysis. Getting the best from ECMO requires early and rapid identification of cardiogenic shock and emergency transfer of the patients to an expert centre before
intensetimes issue 12. Spring 2011
the development of MOF. This in turn implies the availability of a mobile unit to transfer unstable patients, with resultant costs. Beyond ECMO Total artificial hearts such as the CardioWest™ (SynCardia Systems) are expensive and bulky and come into their own only when longer-term assistance is needed. Emerging technologies are led for the moment by implantable continuous-flow pumps such as the HeartMate® (Thoratec) (see Slaughter MS et al. N Engl J Med 2009;361:2241–51. Bridge to whatever Traditionally, the use of mechanical-assist devices has been described as providing a „bridge‟ to recovery or transplantation, or as an end in itself („destination bridging‟). Professor Combes suggested that it is now appropriate to explicitly widen the range of possible destinations: he proposed that mechanical assistance should be described as a bridge to whatever is in the patient‟s best interests – including withdrawal of therapy.
aSHOCK investigators themselves appear to have come to a different conclusion. Noting that low SVR preceded a diagnosis of culture-positive sepsis by several days they interpreted their data as an indication of low SVR disposing to infection rather than infection leading to low SVR. This is not necessarily incompatible with the idea that sepsis (or SIRS) may then prohibit compensatory vasoconstriction. bTreatment was administered according to a protocol that emphasized avoidance of vasopressors. ISICEM, 22 March Session: Severe heart failure intensetimes issue 12. Spring 2011 Panel .
Definitions of some cardiac function indices discussed in the text. See page 2 et seq. for details. LV = left ventricle; EDA = end-diastolic area; ESA = end-systolic area. Cardiac function index (min-1) intensetimes issue 12. Spring 2011 Figure A.
A depiction of the some principles involved in evaluation of ventricular contractility in a setting of optimized ventricular-arterial coupling. See page 3 for further details of this method and the clinical significance of the Ea/Ees ratio. Ea = arterial elastance; Ees = end-systolic ventricular elastance; SV = stroke volume; ESP = end-systolic pressure.
Die Behandlung der Tuberkulose T U B E R K U L O S E Kranke mit offener Tuberkulose werden auf geschlossenen Spitalab- Das Wesen dieser Krankheit teilungen von Pflegepersonen mit Mundschutz und Handschuhen be-handelt bis sie keine Bakterien mehr streuen. Danach werden sie am-Der Erreger dieser Erkrankung ist ein Bakterium, das Mycobacterium bulant weiter therapiert wie die Erkrankte
Arch. Environ. Contam. Toxicol. 48, 242–250 (2005)DOI: 10.1007/s00244-003-0262-7Comparative Sublethal Toxicity of Nine Pesticides on Olfactory LearningPerformances of the Honeybee Apis melliferaA. Decourtye,1 J. Devillers,2 E. Genecque,3 K. Le Menach,4 H. Budzinski,4 S. Cluzeau,1 M. H. Pham-Delgue31 Association de Coordination Technique Agricole, Maison des Agriculteurs, La Tour de Salvag



 intensetimes issue 12. Spring 2011
intensetimes issue 12. Spring 2011 
 intensetimes issue 12. Spring 2011
intensetimes issue 12. Spring 2011 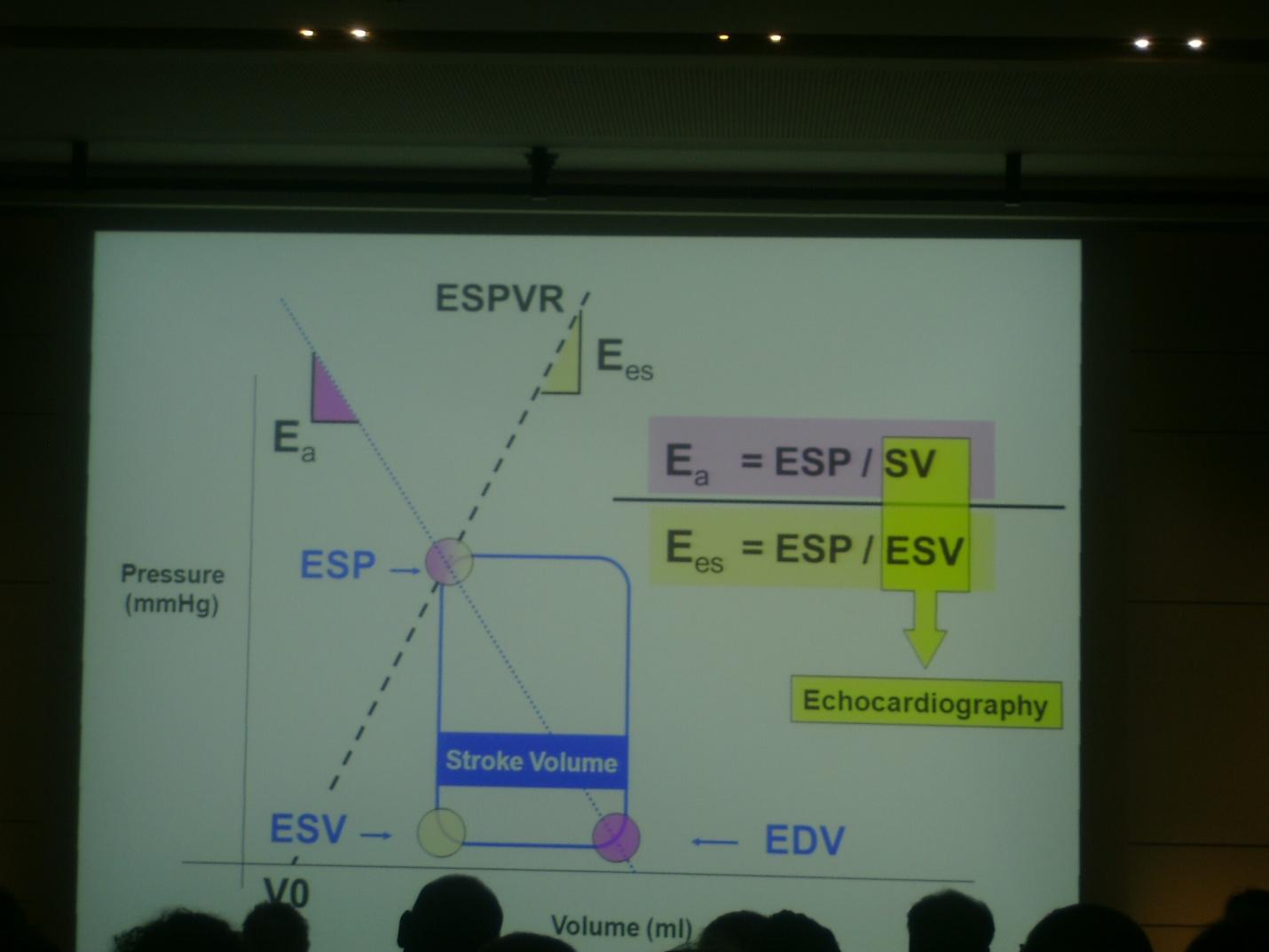 intensetimes issue 12. Spring 2011
intensetimes issue 12. Spring 2011