The wager 9(35): bupropion in the treatment of pathological gambling
The Wager 9(35): Bupropion in the Treatment of Pathological Gambling
Volume 9 Number 35 - September 1, 2004 Treating the Source, the Symptoms, or the Correlates? Bupropion in the Treatment of Pathological Gambling
Chemical treatments abound in today’s society for almost
any condition or perceived deficit. Whether it involves
taking diet pills to lose weight, anti-depressants to fight
the blues, or Ginkgo to improve memory, we often look to
medication (of greater or lesser scientific merit) for a
solution to our problems. However frivolously they have
been used elsewhere, pharmacological treatments have
had significant impact on the chemical addictions.
Recovering heroin users have been taking methadone
since the 1970’s and people who are trying to quit
smoking can take Zyban to reduce cravings and
withdrawal symptoms. But what about treatment for
pathological gambling (PG), a non-substance-related
addiction? If PG was as responsive to chemical treatments
as nicotine dependence and heroin dependence appear to
be, this evidence would support the idea that behavioral
addictions are analogous to substance-related addictions.
While pharmacological treatment is new territory for PG
patients, several studies have already been conducted
examining the efficacy of drug therapy. A recent
preliminary study conducted by Black (2004) tested the
efficacy of the psychostimulant bupropion (Wellbutrin) for
As a psychostimulant, bupropion is used primarily to treat
attention deficit hyperactivity disorder (ADHD). Specker
http://www.thewager.org/current.htm (1 of 5) [9/7/2004 8:52:54 AM]
The Wager 9(35): Bupropion in the Treatment of Pathological Gambling
and colleagues (1995) found a high comorbidity between
PG and ADHD, leading them to believe the ADHD
symptoms of impulsivity and attention deficit might make
individuals more vulnerable to substance abuse and PG.
This suspected link influenced Black’s choice of bupropion
Black used advertisements to recruit ten subjects (six
women and four men) who had scores of >=5 on the
South Oaks Gambling Screen (SOGS) and met DSM-IV
criteria for PG with symptoms lasting for at least one year.
A diagnosis of ADHD was not required for inclusion – only
one subject met criteria for ADHD. Subjects who had
current diagnoses of schizophrenia, anxiety disorders,
bipolar disorders, eating disorders, seizure disorders, or
substance use disorders were excluded from participating
in the study. At baseline and each week during the eight-
week study, subjects completed: a) the Yale- Brown
Obsessive-Compulsive Scale Pathological Gambling Version
(YBOCS-PG) to determine the severity of PG; b) the
Attention Deficit Hyperactivity Disorder (ADHD) checklist
to measure symptoms of ADHD; c) the Hamilton Rating
Scale for Depression (HRDS); d) the Clinical Global
Impression Inventory (CGI) to measure gambling
symptom improvement; and e) the Sheehan Disability
Scale (SDS) to assess disability in their family, social, and
work lives. Black started subjects with a dosage of 100 mg
daily of slow release bupropion, increased the daily dose
by 100 mg each week for three weeks, and then had
subjects maintain a steady dosage for 5 more weeks.
Figure 1: Changes in Assessment Scores during 8-week Bupropion Treatment
http://www.thewager.org/current.htm (2 of 5) [9/7/2004 8:52:54 AM]
The Wager 9(35): Bupropion in the Treatment of Pathological Gambling
* = significant difference (p < .01) on paired t-test, baseline to endpoint. Note. Assessments are ordered according to effect size. Three subjects did not complete
the week 6 and week 8 visits. Their week 4 scores were counted as their end point
As shown in Figure 1, between baseline and end point
(i.e., week 8 for seven subjects and week 4 for three
subjects), subjects’ PG severity (according to both the
YBOCS and the CGI), ADHD scores, and work and family
life disabilities significantly decreased. Seventy percent of
the sample reported gambling symptoms as “very much
Subjects showed significant improvement on five of seven
assessments from baseline to end point; however, this
study has several limitations. It is a preliminary study of a
small number of subjects that lacks a placebo control
condition. The lack of a control group makes it impossible
to rule out a placebo effect as the primary contributor to
http://www.thewager.org/current.htm (3 of 5) [9/7/2004 8:52:54 AM]
The Wager 9(35): Bupropion in the Treatment of Pathological Gambling
Despite its limitations, this preliminary study is the first to
explore the effectiveness of a psychostimulant in treating
PG; the results encourage more rigorous research on
pharmacological therapies for the treatment of PG. There
have been studies on other medications for the treatment
of PG that also showed efficacy. Kim et al. (2001)
conducted a double-blind placebo-controlled study of 45
patients testing the efficacy of naltrexone (commonly used
to treat alcoholism or opiod dependence) for the treatment
of PG and found that 75% of the subjects on naltrexone
compared to 24% of the placebo subjects had improved
CGI scores. Another double-blind study by Hollander et al.
(2000) found that the selective serotonin reuptake
inhibitor (SSRI) fluvoxamine (most commonly used to
treat obsessive compulsive disorder) was an effective
treatment for PG (see for a review of Hollander’s preliminary study).
The results of these studies cited above suggest that
pathological gamblers respond to different types of
pharmacological treatment because pathological gamblers
as a group include people with a variety of underlying
antecedents or correlates of PG (e.g., depression,
substance abuse, or ADHD). The study outcomes also
contribute to the evidence that pharmacological
treatments can be applied successfully to behavioral as
well as chemical addictions. These findings have
implications for the way we understand addiction. Both
chemical and behavioral treatments appear to have similar
efficacy in treating chemical and behavioral addictions, and
both behavioral and chemical addictions share similar
behavioral and neurochemical antecedents and
consequences. Therefore, the distinction between the
chemical and behavioral addictions and their treatment
might be a less important distinction than variations in
other aspects of addiction (e.g., comorbid conditions).
Comments on this article can be addressed to Alexa
http://www.thewager.org/current.htm (4 of 5) [9/7/2004 8:52:54 AM]
The Wager 9(35): Bupropion in the Treatment of Pathological Gambling
References
Black, D. W. (2004). An open-label trial of bupropion in
the treatment of pathologic gambling. Journal of Clinical Psychopharmacology, 24(1), 108-110.
Hollander, E., DeCaria, C. M., Finkell, J. N., Begaz, T.,
Wong, C. M., & Cartwright, C. (2000). A randomized
double-blind fluvoxamine/placebo crossover trial in
pathologic gambling. Biological Psychiatry, 47(9), 813-
Kim, S. W., Grant, J. E., Adson, D. E., & Shin, Y. C.
(2001). Double-blind naltrexone and placebo comparison
study in the treatment of pathological gambling. Biological
Specker, S. M., Carlson, G. A., Christenson, G. A., &
Marcotte, M. (1995). Impulse control disorders and
attention deficit disorder in pathological gamblers. Annals of Clinical Psychiatry, 7(4), 175-179.
Copyright 2004 the President and Fellows of Harvard College
http://www.thewager.org/current.htm (5 of 5) [9/7/2004 8:52:54 AM]
PROF 42 69355/11/03 30/1/04 11:12 am Page 14Faculty of Dental SurgeryClinical guideline summaries - Fourth edition Professor Fraser McDonald is Chairman of the Faculty of Dental Surgery Clinical Effectiveness Committee. Professor McDonald’s undergraduate qualification was completed in 1980 at Birmingham University. He has subsequently obtained qualifications in specialisation
FORBEREDELSER Før jeg reiste tok jeg noen vaksiner som ble anbefalt på helsestasjonen og kjøpte noen norskelegemidler som jeg ble anbefalt å ta med (Paracet, Zyrtec, Imodium og noe annet som jeg bleanbefalt på helsestasjon). Hadde ikke noe bruk for noe av dette og tror jeg også hadde klartmedfint uten vaksinene. Vaksinene kostet ca 1000kr og noen av di bør settes i god tid før manreiser.
 The Wager 9(35): Bupropion in the Treatment of Pathological Gambling
Volume 9 Number 35 - September 1, 2004
The Wager 9(35): Bupropion in the Treatment of Pathological Gambling
Volume 9 Number 35 - September 1, 2004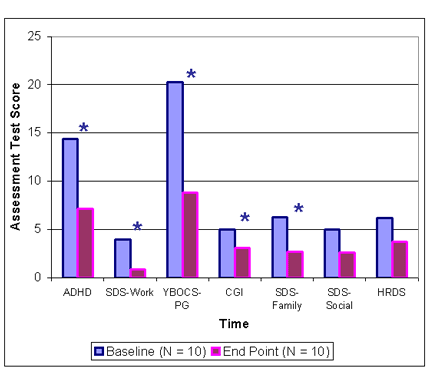 The Wager 9(35): Bupropion in the Treatment of Pathological Gambling
* = significant difference (p < .01) on paired t-test, baseline to endpoint.
The Wager 9(35): Bupropion in the Treatment of Pathological Gambling
* = significant difference (p < .01) on paired t-test, baseline to endpoint.