START-1 TRIAL After survey completion, please give to Dr. or Office Staff for submission. Thank you. TO PHYSICIAN OR OFFICE STAFF--- Upon Completion, please Fax or Upload completed survey to: Clarity Research To Submit Via Fax: 1-888-389-9193 To Submit Via Website Portal: www.crcsciences.com Clarity Research and Consulting STUDY ID: START-1 PRACTICE Code: ____ Patient ID: ______________ MALE or FEMALE
1. PRIMARY COMPLAINT/DIAGNOSIS (Circle all that apply)
Arthritis
Feet Hips Knees Neck Shoulders Back Other
Neuropathy or Radiculopathy (Radiating Pain)
Myofascial/ Musculoskeletal Pain or Spasm
Tendinitis
o Other __________________________
STUDY ID: START-1 Trial Brief Pain Inventory (Short Form)
Pt ID: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Throughout our lives, most of us have had pain from time to time (such as minor
headaches, sprains, and toothaches). Have you had pain other than these every-
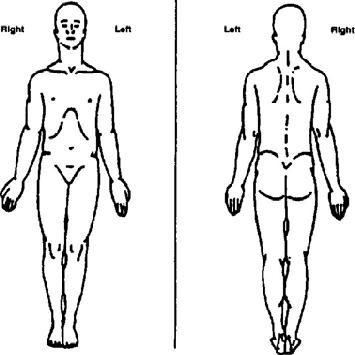
On the diagram, shade in the areas where you feel pain. Put an X on the area that
Please rate your pain by circling the one number that best describes your pain at its
Please rate your pain by circling the one number that best describes your pain at its
Please rate your pain by circling the one number that best describes your pain on
Please rate your pain by circling the one number that tel s how much pain you have
STUDY ID START-1 Trial
PT. ID: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
What treatments or medications are you receiving for your pain?
NO ANSWER NEEDED HERE- PLEASE SKIP
In the last 24 hours, how much relief have pain treatments or medications
provided? Please circle the one percentage that most shows how much relief
you have received. 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Circle the one number that describes how, during the past 24 hours, pain has
Normal Work (includes both work outside the home and housework)
CURRENT MEDICATION USAGE (CHECK ALL THAT APPLY) Over-the-Counter (OTC) Pain Medication o Advil®, Motrin® (ibuprofen) o ALEVE® (naproxen o Aspirin (acetylsalicylic acid) o Tylenol® (acetaminophen) o Other If you have indicated any medications taken above—What is Dose and How often per day? Anti-Inflammatory (Prescription) o Anaprox (naproxen sodium) o Dolobid (diflunisal) o Naprosyn (naproxen) o Celebrex (celecoxib) o Feldene (piroxicam) o Relafen (nabumetone) o Clinoril (sulindac) o Indocin o Toradol (ketorolac tromethamine) (indomethacin) o Daypro (oxaprozin) o Lodine (etodolac) o Vimovo (naproxen/esomeprazole) o Disalcid (salsalate) o Mobic (meloxicam) o Voltaren (diclofenac) If you have indicated any medications taken above—What is Dose and How often per day? Narcotic o Avinza®, Kadian® (morphine) o Lorcet®, Lortab®, Norco®, Vicodin® (hydrocodone) o Demerol meperidine o Opana® (oxymorphone) o Dilaudid®, Exalgo® (hydromorphone) o Oxycontin®, Oxyfast®, Percocet®, Roxicodone® (oxycodone and acetaminophen) o Duragesic®, Fentora®, Actiq® (fentanyl) Neurontin® (gabapentin) Lyrica® (pregabalin) Ultram® (tramadol) If you have indicated any medications taken above—What is Dose and How often per day?
Dismenol forte Ibuprofen 400 mg-Filmtabletten GEBRAUCHSINFORMATION: INFORMATION FÜR DEN ANWENDER Dismenol forte Ibuprofen 400 mg-Filmtabletten Lesen Sie die gesamte Packungsbeilage sorgfältig durch, denn sie enthält wichtige Informationen für Sie. Dieses Arzneimittel ist ohne Verschreibung erhältlich. Um einen bestmöglichen Behandlungserfolg zu erzielen, muss Dismenol forte I
Tillæg til Cardiologisk Forum Oktober 2002 Nye retningslinjer vedrørende diagnostik og behandling Olav W.Nielsen, Niels Gadsbøll, Lars Køber, Per Hildebrandt, Henrik Villadsen Fra Arbejdsgruppen om Hjerteinsufficiens under Dansk Cardiologisk Selskab Introduktion 2. Objektiv dokumentation for kardial dysfunktionI 2001 udkom en task-force rapport om diagnostik3. Ved tvivl kan diagnosen
 STUDY ID: START-1 Trial
STUDY ID: START-1 Trial