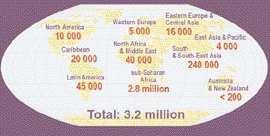
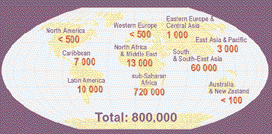
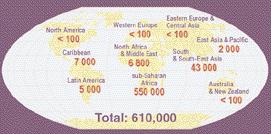
Breast feeding and HIV transmission: Current state of the evidence Robert Pratt BA, MSc, RN, RNT, FRCN, Professor of Nursing, Richard Wells Research Centre, Thames Valley University London Carol Pellowe BA (Hons), MA (Ed), RN, RNT, Principal Lecturer (Research), Richard Wells Research Centre, Thames Valley University London Women now account for at least half of the total global number of adults living with HIV/AIDS. Most of them are of childbearing age and, as more and more women have become infected with HIV, an increasing number of their newborn infants are also at risk of becoming infected from them before, during or soon after childbirth. This article looks at the feasibility of preventing mother-to-child transmission of HIV, particularly in the industrially developing regions of the world. Keywords: breast feeding; breast milk; human immunodeficiency virus; vertical transmission; prevention Introduction By the beginning of 2003, more than 3.2 million children under the age of 15 years throughout the world were living with HIV/AIDS (Figure 1). During the previous year, more than 800,000 children were newly infected with HIV (more than 2,250 every day) and at least 1,700 children died every day (Figures 2 and 3)(UNAIDS/WHO, 2002).
Figure 3. Estimated number of children (<15 years) newly infect-ed with HIV during 2002. Courtesy of UNAIDS (2002).
may soon dwarf the current tragedy being experienced today insouthern Africa. In addition, the force of national epidemics ofHIV infection in resource-poor countries in eastern Europecontinue to build, setting the stage for increased risk tochildren (UNAIDS/WHO, 2002).
In contrast in the richer nations of the industrially
Figure 1. Children (<15 years) estimated to be living with HIV-
developed world, comprehensive prevention strategies have
AIDS as of end 2002. Courtesy of UNAIDS (2002).
dramatically decreased the number of HIV-infected newbornchildren to the point where it is becoming uncommon forchildren to become infected from their mothers.
Key points Pratt, R. and Pellowe, C. (2003) Breast feeding and HIV
transmission: Current state of the evidence. Journal ofNeonatal Nursing 9(4): 133-39.
1. Over 800 000 children throughout the world acquire HIV
infection from their mothers every year.
2. Those children living in the impoverished countries of
Figure 2. Estimated deaths in children (<15 years) from HIV/AIDS
the developing world are at greatest risk of infection.
during 2002. Courtesy of UNAIDS (2002).
3. There is conclusive evidence that HIV is transmitted by
The risk of becoming infected with HIV depends mainly on
4. Modification of infant feeding practices, where appropri-
where the child is born. Most HIV-infected children (90%) are
ate, can significantly reduce the risk of mother-to-child
born in impoverished countries in the industrially developing
world, mainly sub-Saharan Africa. However, as national HIV
5. For most newborn children in the developing world,
epidemics escalate in South and Southeast Asia, the number of
breast feeding should continue to be recommended and
HIV-infected infants born in these densely populated regions
JOURNAL OF neonatal NURSING VOLUME 9 ISSUE 4 2003
Breast feeding and HIV transmission 133 Maternal Factors
Primary HIV infection and symptomatic HIV disease, both associated with high levels of HIV in the plasma (viral load) and low numbersof CD4+ T-lymphocytes, are associated with an increased risk for MTCT (Garcia et al, 1999; Anderson, 2001).
High plasma and genital tract viral load is associated with an increased risk for MTCT (Garcia et al, 1999; Anderson, 2001; Fang et al, 1998).
Low CD4+ T-lymphocyte count or decreased CD4+:CD8+ ratio are both associated with an increased risk for MTCT (Anderson, 2001).
Antiretroviral treatment and prophylaxis
The use of antiretroviral drugs (zidovudine, lamivudine, nevirapine) in treatment regimens for the mother or as chemoprophylaxis for the neonate have been shown to significantly decrease the risk for MTCT (Anderson, 2001).
Vitamin A deficiency is associated with an increased risk of pre-term delivery which increases the risk of MTCT (Coutsoudis et al, 1999a). Severe deficiency may also adversely affect the integrity of the vaginal mucosa and increase HIV vaginal shedding (John et al, 1997).
A history of unprotected penetrative sexual intercourse with several partners has been associated with an increased risk for MTCT (Anderson, 2001; Bulterys et al, 1997).
The presence of other sexually transmitted infections increases plasma viraemia (viral load). These infections also increase the number of genital tract inflammatory cells which stimulates HIV shedding, increasing the risk for MTCT (Anderson, 2001; Plummer, 1998).
The use of illicit drugs during pregnancy increases the risk for MTCT(Anderson, 2001; Rodriguez et al, 1996; Lyman, 1993).
Obstetric Factors
Pre-term delivery has been shown to increase the risk for MTCT. (Anderson, 2001; Kuhn et al, 1997; Kuhn et al, 1999)
The risk of MTCT increases linearly with increasing duration of ruptured membranes with a 2% increase in risk for each hour increment. Women with late symptomatic HIV disease (AIDS) have a31% probability of MTCT after 24 hours of ruptured membranes. (Read, 2000)
Placental disruption-abruption, chorioammionitis
Chorioammionitis increases the risk of MTCT (Goldenbert et al, 1998) and placental abruption causing disruption of the placental-fetal barrier, may increase fetal exposure to maternal blood and increases the risk of MTCT (Anderson, 2001).
Use of fetal scalp electrodes, fetal scalp sampling, amnioscopy and amniocentesis increases the risk for MTCT (Maiques et al, 1999; Mandelbrot et al, 1996).
Use of episiotomy, vacuum extraction or forceps may increase the risk for MTCT by exposing the fetus to maternal blood and genital secretions. However, careful use may shorten duration of labour or ruptured membranes with vaginal delivery and this may decrease risk of MTCT (Anderson, 2001). External version should be avoided because of the increased risk for maternal-fetal bleeding.
Caesarean delivery performed before the onset of labour and rupture of membranes can reduce the risk of MTCT by 55-88% (EMDC, 1999; IPHIVG, 1999). Postnatal factors
The risk of MTCT from breast feeding is greatest in early infancy (before 6 months of age) and persists as long as breast feeding continues (Miotti et al, 1999; Nduati et al, 2000; John et al, 2001). The longer the duration of breast feeding, the greater the risk of MTCT(Leroy et al, 1998; Embree et al, 2000; Read et al, 2002).
Mothers may initially become infected with HIV as a result of an unscreened blood transfusion during the peripartum period. During maternal primary HIV infection, when the plasma viral load is high, there is a significantly increased risk for MTCT from breast feeding.
Table 1. Factors that influence the risk for MTCT of HIV
134 Breast feeding and HIV transmission
JOURNAL OF neonatal NURSING VOLUME 9 ISSUE 4 2003
Prevent further sexually transmitted infections during pregnancy by reducing the number of sexual partners
Reduce the frequency of unprotected sexual intercourse
Discontinue the use of illicit drugs during pregnancy
Commence mother on antiretroviral therapy or
Effectively treat any co-existing sexually transmitted infections
If vitamin A deficient, provide vitamin supplementation
Avoid invasive tests or monitoring during the antenatal and intrapartum period
Consider the benefits of caesarean delivery
Cease breast feeding as early as possible
Use only blood and blood components that have been screened for HIV infection
Table 2. Methods for preventing MTCT. Mother-to-child transmission
becoming infected in the first place. All other interventionsdesigned to prevent newborn children becoming infected from
Mother-to-child transmission (MTCT), also known as vertical
their mothers depend upon maternal infection being detected
or perinatal transmission, can occur during pregnancy (in
before the child is born. Antenatal screening for HIV infection
utero), during birth (intrapartum) when the newborn infant
is an essential element of a comprehensive strategy for
comes into contact with infected maternal birth fluids during
preventing women giving birth to HIV-infected children (Pratt,
the birth process, and shortly after birth (postpartum) or
during the early months of life while being breast fed. Most
European Consensus Guidelines on the management of
children (75%) become infected during the peripartum
HIV infection during pregnancy (Newell and Rogers, 2002) are
period, i.e. during or shortly after delivery (Microchnick et al,
available and these are summarised in Table 3. UK-specific
guidelines(Lyall et al, 2001) are also available and regularlyupdated and these can be downloaded from the internet at:
Risk factors
http://www.bhiva.org/guidelines.htm Finally, guidelines from
Women are potentially at risk of initial infection during sexual
the USA National Institutes for Health (NIH, 2002) are
intercourse with HIV-infected men, from sharing HIV-
available as a ‘Living Document’ on the internet at:
contaminated injecting equipment, or following treatment with
http://www.aidsinfo.nih.gov/guidelines/perinatal/Perinatal.pdfAll three of these guidelines are in general agreement on how
transfusions of unscreened whole human blood or blood
best to prevent MTCT of HIV and nurses, midwives and other
healthcare professionals working within this field need to be
Once infected, several maternal, obstetric and postnatal
familiar with their recommendations and advice.
factors can increase the likelihood of mothers transmitting HIVinfection to their child before, during and immediatelyfollowing birth. Some of the most important risk factors are
Risk to infants of HIV transmission
described in Table 1 and further discussed elsewhere (Pratt,
from breast feeding
2003). Understanding these risks has led to the development of
The importance of antenatal screening for HIV infection and
the evidence for the efficacy of antiretroviral chemoprophylaxisand caesarean section delivery for reducing the risk of MTCT
Risk reduction strategies
has previously been described in this journal and
Among the several options that have been described for
elsewhere.(Pratt, 1999; 2000; 2003) However, there remains
preventing MTCT (Table 2)(Pratt, 1999; 2003) the following
some confusion over the recommendations(Newell and
Rogers, 2002; Lyall et al, 2001; NIH, 2002) for modifying infant
feeding practices to prevent viral transmission.
There are considerable advantages to both mother and
infant in breast feeding, especially during the first six months
• mothers refraining from breast feeding
of life. Throughout the world, breast feeding protects against
In western Europe, where these interventions are available, the
respiratory infections and diarrhoeal disease, two of the most
rate of MTCT has fallen from an average of 15% to 2% or less
important causes of childhood mortality, and it has significant
by 1999(ECS, 2001). This pattern is replicated in other
economical, social, psychological and family planning
advantages. However, in HIV-infected mothers, both cell-free
Equally important, any effective strategy aimed at reducing
and cell-associated virus have been consistently identified in
the risk of MTCT must first focus on preventing women from
colostrum and mature milk and the transmission of HIV in
JOURNAL OF neonatal NURSING VOLUME 9 ISSUE 4 2003
Breast feeding and HIV transmission 135
All pregnant women, and ideally, those planning a pregnancy, are offered and recommended to have an HIV test. HIV testing should also be offered to their sexual partner(s).
HIV-infected women should be given the option of delivering their child through a CS performed before labour and before rupture of membranes (usually at 38 weeks’ gestation).
All HIV-infected women should be offered therapy during pregnancy fortheir own health depending on their clinical status and prognostic markers.
Antiretroviral treatment can begin after the first trimester.
Most antiretroviral drugs have not been shown to be associated with an increased risk for birth defects (teratogenicity) except efavirenz, zalcitabine and hydroxyurea, which are contraindicated during pregnancy.
A 3-part zidovudine (ZDN) regimen is used as the standard chemoprophylaxis to prevent MTCT; ZDN is given during pregnancy, during labour and in the neonatal period, commencing at 28-32 weeks’ gestation (with elective CS delivery at 38 weeks gestation).
If CS delivery is not an option, in addition to ZDN:
two doses of nevirapine may be given once labour has been established
lamivudine (3TC) may also be given with ZDN
HIV-infected women are strongly advised to refrain from breast feeding where safe infant-feeding alternatives are available.
Women who cannot refrain from breast feeding should be advised to:
Exclusively breast feed and not introduce other foods or drinks for4-6 months;
Breast feed for as short a time as possible, with rapid cessation.
Follow-up of children born to HIV-infected mothers
Long-term follow-up of all children born to HIV-infected mothers should continue, at least until school age.
Table 3. Summary of European Consensus Guidelines on the Management of HIV Infection in Pregnancy (Newall and Rogers, 2002).
breast milk, occurring at any point during lactation, has been
life (Fautaini, 1997; Simonon at al, 1994).
Avoidance of breast feeding and the use of breast milk
Several factors are involved in or associated with HIV
substitutes will substantially reduce postnatal mother-to-child
transmission via breast milk. High levels of maternal viraemia
HIV transmission and this strategy is recommended in
(high viral load) will increase the amount of HIV secreted in
industrialised countries, including the UK, where safe
breast milk and, consequently, increase the amount and
alternatives to breast feeding are available (Newell and Rogers,
duration of HIV exposure to the infant. Vitamin A deficiency in
2002; Lyall et al, 2001; NIH, 2002). Globally, however, most
HIV-infected mothers is associated with cracked nipples (and
infants at risk of postnatal mother-to-child HIV transmission
increased vaginal shedding of HIV) which may be an additional
are breast fed. In many cultures and in many regions of the
source of viral exposure to the infant (John et al, 1997). Infant
developing world, it is neither possible nor acceptable for
prematurity results in an immature neonatal immune system
unable to mount an effective cell-mediated response to HIVand is associated with an increased risk of viral acquisition from
Exclusive breast feeding
breast feeding (John et al, 1997; Ekpini et al, 1997).
The actual mechanism of HIV transmission by breast milk is
Studies conducted in South Africa found evidence that women
not fully understood. However, neonatal mucus membranes
who exclusively breast feed had a lower rate of MTCT than
cannot effectively prevent HIV infection and exposure to HIV
those mothers who also fed their babies other fluids or food
in breast milk may result in viral infection directly through oral
together with breast feeding (mixed infant feeding)
and gastric mucosa (Nduati, 1998). Other conditions that may
(Coutsoudis et al, 1999b; 2001). Potential mechanisms that
disrupt the integrity of neonatal oral mucosa, e.g., candidiasis,
might explain a reduced risk for MTCT when children are
have been associated with an increased risk of HIV infection
exclusively breast fed include (Smith and Kuhn, 2000)
• reduction in dietary antigens and enteric pathogens from
The amount of HIV secreted in breast milk is highest during
fluids and food, helping to maintain the integrity of the
the first few months following delivery and 70% of postnatal
intestinal mucosal barrier and limit the inflammatory
transmission takes places within the first four to six months of
136 Breast feeding and HIV transmission
JOURNAL OF neonatal NURSING VOLUME 9 ISSUE 4 2003
• promotion of beneficial intestinal microflora that may
HIV-infected woman and children must be part of the regular
increase resistance to infection and enhance the infant’s
programme so that staff can feel confident and competent to
care for and support these mothers and their infants in the best
• the beneficial antimicrobial, anti-inflammatory and
immuno-modulating properties of breast milk.
Conclusion
Consequently, if there are no consistently safer alternatives to
In most countries, the children of HIV-infected mothers will
breast feeding for HIV-infected mothers, exclusive breast
find themselves born into a world where they are immediately
feeding is the second best option for reducing the risk of
disadvantaged. Most will eventually be orphaned as the result
MTCT in the postnatal period. However, it must be realised
of the AIDS-related deaths of their parents and by 2010, more
that many mothers in resource poor countries of the world,
than 25 million children are projected to lose one or both
suffering malnutrition and poor health themselves, may not
parents due to HIV disease (USAID, 2002). The majority of
produce enough breast milk to be able to exclusively breast
these children will be stigmatised, impoverished and deprived
feed their babies and they will manage the best they can by
of even basic needs for food, water, shelter and protection.
Their chances of survival will be diminished even further if theyhave also become infected from their mothers before, during
Practical considerations
With the current emphasis on breast feeding in UK maternity
In this discussion we have seen that we have the ability to
units, it is important that women choosing to bottle feed do not
prevent MTCT of HIV to infants. However, the necessary
feel stigmatised (DoH, 2003; UNICEF, 2003). African women
counselling, testing and treatment needed to do this is
resident in the UK, and women from many other ethnic
hampered by a geographical lottery, where children born in
groups, traditionally breast feed their babies. A decision to
countries with poorly organised and starkly under-resourced
bottle feed, especially if associated with a delivery by caesarean
prenatal healthcare services will be at most risk. Already
section, may raise suspicion of their HIV status among other
millions of children have been infected and thousands more
members of their family, neighbours and in their community.
are becoming infected every day (UNAIDS/WHO, 2002).
Because of this, it is important that the decision about infant
References
feeding is raised as soon as a diagnosis of maternal HIVinfection is known and neonatal nurses and midwives
Anderson, J.R. (2001) HIV and Reproduction. In: Anderson JR, ed.
specialising in the care of HIV positive women are well placed
A Guide to the Clinical Care of Women with HIV. Washington
DC: U.S. Department of Health and Human Services, Health
Woman may associate not breast feeding with not being a
Resources and Services Administration, HIV/AIDS Bureau; 7:
good mother and time needs to be given to explore such
feelings. The mother also needs time to prepare a story as to
Bulterys, M., Landseman, S., Burns, D.N., Robinstein, A., Goedert,
why she is not breast feeding. A plausible excuse needs to be
J. (1997) Sexual behavior and injection drug use during pregnan-
developed, such as an illness during pregnancy or inadequate
cy and verticial transmission of HIV-1. Journal of the Acquired
lactation, and the mother needs to rehearse this and feel
Immune Deficiency Syndrome and Human Retrovirology 15:76-82. Coutsoudis, A., Pillay, K., Spooner, E., Khun, L., Coovadia, H.M.
In the postnatal period, staff need to adopt a positive
(1999a) Randomized trial testing the effect of vitamin A supple-
approach to bottle feeding and offer appropriate support. This
mentation on pregnancy outcomes and early mother-to-child
includes establishing bottle feeding and the making up of
HIV-1 transmission in Durban, south Africa. South African
feeds. If the mother has limited finances, as in the case of
Vitamin A Study Group. AIDS 13:1517-24.
asylum seekers, assistance may be needed to acquire the
Coutsoudis, A., Pillay, K., Spooner, E., Kuhn, L., Coovadia, H.M.
necessary equipment. Prior to discharge home, many maternity
(1999b) Influence of infant-feeding patterns on early mother-to-
units are able to provided limited supplies of formula milk and
child transmission of HIV-1 in Durban, South Africa: a prospec-tive cohort study. South African Vitamin A Study Group.
equipment needed to sterilise bottles and other equipment. 354(9177):471-76.
However, nursing or midwifery staff should ensure the mother
Coutsoudis, A., Pillay, K., Kuhn, L., Spooner, E., Tsai, W.Y.,
has access to the necessary funds to support consistent bottle
Coovadia, H.M. (2001) Method of feeding and transmission of
feeding and knows where to purchase future supplies. Failure
HIV-1 from mothers to children by 15 months of age: Prospective
to do so could result in the mother resorting to mixed infant
cohort study from Durban, South Africa. AIDS 15(3):379-87.
feeding, the dangers of which have already been described. Department of Health. (2003) Getting the right start. National
At all times confidentiality about the woman’s HIV status
Service Framework for Children: Standard for Health Services.
must be maintained. Unfortunately, anecdotal reports about
Ekpini, E., Wikto, S.Z., Satten, G.A. et al. (1997) Late postnatal
staff not maintaining patient confidentiality continue to occur.
transmission of HIV-1 in Abidjan, Côte d’Ivoire. Lancet 349:1054-
Although the risk of MTCT can be significantly reduced by the
interventions described in this paper, in some instances, infants
Embree, J.E., Njenga, S., Datta P. et al. (2000) Risk factors for post-
will still become infected. Consequently, the postnatal period is
natal mother-to-child transmission of HIV-1. AIDS 14(16):2535-41.
an anxious time for parents as they await the results of HIV
European Collaborate Study. (2001) HIV-infected women and verti-
cal transmission in Europe since 1986. AIDS 15:761-70.
In-service educational sessions that address issues about
European Mode of Delivery Collaboration. (1999) Elective caesare-
JOURNAL OF neonatal NURSING VOLUME 9 ISSUE 4 2003
Breast feeding and HIV transmission 137
an-section versus vaginal delivery in prevention of vertical HIV-
mission through breastfeeding: A study in Malawi. Journal of the
transmission: A randomised clinical trial. Lancet 353:1035-9. American Medical Association 282:744-49. Fang, G., Burger, H., Anastos, K. et al. (1998) Sequence analysis of Mirochnick, M., Fenton, T., Gagnier, P. et al. (1998)
the complete HIV-1 pol gene from virions in plasma and genital
Pharmacokinetics of nevirapine in human immunodeficiency
tract of women: Genital tract reservoir and differential drug resis-
virus type 1- infected pregnant women and their neonates. Journal
tance. HIV Pathology and Treatment Conference. Abstracts (Abst
of Infectious Diseases 1998; 178:368-74. National Institutes of Health (Perinatal HIV Guidelines Working Fantaini, J., Yahi, C., Delezay, O., Tamalet, C. (1997) HIV transmis- Group). (2002) Revisions to the February 4, 2002 Public Health
sion across the vaginal epitheliums. AIDS 11:1663.
Service Task Force Recommendations for the use of antiretroviral
Garcia, P.M., Kalish, L.A., Pitt, J. et al. (1999) Maternal levels of
drugs in pregnant women infected with HIV-1 for maternal
plasma human immunodeficiency virus type-1 RNA and the risk
health and for reducing perinatal HIV-1 transmission in the
of perinatal transmission. New England Journal of Medicine 341:394-
http://www.aidsinfo.nih.gov/guidelines/perinatal/Perinatal.pdf
Goldenbert, R.L., Vermund, S.H., Soepfert, A.R., Andrews, W.W. Nduati, R. (1998) HIV and Infant Feeding: A Review of HIV
(1998) Choriodecidual inflammation. A potentially preventable
Transmission Through Breastfeeding 1998. WHO/FRH/NUT
cause of perinatal HIV-1 transmission? Lancet 352:1927-30. International Perinatal HIV Group. (1999) The mode of delivery Nduati, R., John, G., MboriNgacha, D. et al. (2000) Effects of
and the risk of vertical transmission of human immunodeficiency
breastfeeding and formula feeding on transmission of HIV-1: A
virus type-1. New England Journal of Medicine 340:977-87.
randomized clinical trial. Journal of the American Medical AssociationJohn, G.C., Nduati, R.W., Mbori-Ngacha, D. et al. (1997) Genital 283: 1167-74.
shedding of human immunodeficiency virus type 1 DNA during
Newell ML, Rogers R, eds. (2002) Pregnancy and HIV Infection: a
pregnancy: Association with immunosuppression, abnormal cervi-
European Consensus on Management. AIDS 16(Suppl 2):S1-S-18.
cal and vaginal discharge and severe vitamin A deficiency. JournalPlummer, F.A. (1998) Heterosexual transmission of human immun- of Infectious Disease 175: 57-62.
odeficiency virus type 1 (HIV): Interactions of conventional sexu-
John, G.C., Nduati, R.W., MboriNgacha, D. et al. (2001) Correlates
ally transmitted diseases, hormonal contraception and HIV-1.
of mother-to-child human immunodeficiency virus type 1 (HIV-1)
AIDS Research and Human Retroviruses 14(Suppl 1):S5-10.
transmission: Association with maternal plasma HIV-1 RNA load,
Pratt, R.J. (1999) Perinatal HIV infection in 1999: Effective preven-
genital HIV-1 DNA shedding, and breast infections. Journal of
tative strategies. Journal of Neonatal Nursing 5(2):37-41. Infectious Diseases 183(2):206-12. Pratt, R.J. (2000) Antenatal screening for HIV infection: Removing Kuhn, L., Abrams, E.J., Matheson, P.B. et al. (1997) Timing of
tomorrow’s children from harm’s way. Journal of Neonatal Nursing
maternal-infant HIV transmission: Associations between intra-
6(6):179-84.
partum factors and early polymerase chain reaction results. New
Pratt RJ. (2003) Preventing Mother-to-Child Transmission. In:
York City Perinatal HIV Transmission collaborative Study Group.
HIV&AIDS: A Foundation for Nursing and Healthcare Practice
AIDS 11:429-35. Kuhn, L., Steketee, R.W., Weedon, J. et al. (1999) Distinct risk fac- Read, J. for the International Perinatal HIV Group. (2000)
tors for intrauterine and intrapartum human immunodeficiency
Duration of ruptured membranes and vertical transmission of
virus transmission and consequences for disease progression in
HIV-1: A meta-analysis from fifteen prospective cohort studies.
infected children. New York City Perinatal HIV Transmission
7th Conference on Retroviruses and Opportunistic Infections.
Collaborative Study Group. Journal of Infectious Diseases 179:52-8. Abstracts (Abst 659), January 30-February 02. Leroy, V., Newell, M.L., Dabis, F. et al. (1998) International multi- Read, J.S., Newell, M.L., Dabis, F., Leroy, V. (2002) Breast feeding
centre pooled analysis of late postnatal mother-to-child transmis-
and late postnatal transmission of HIV-1: An individual patient
sion of HIV-1 infection. Ghent International Working Group on
data meta-analysis (Breastfeeding and HIV International
Mother-to-Children Transmission of HIV. Lancet 352(9128):597-
Transmission Study). 15th International AIDS Conference.
Abstracts (Abst TuOrB1177), July 7-12. Lyall, E.G.H., Blott, M., de Ruiter, A. et al. (2001) Guidelines for Rodriguez, E.M., Mofenson, L.M., Chang, B.H. et al. (1996)
the management of HIV infection in pregnant women and the
Association of maternal drug use during pregnancy with maternal
prevention of mother-to-child transmission. British HIV
HIV culture positivity and perinatal HIV transmission. AIDS 10:
Association. HIV Medicine 2 (4):314-30. Available from: Simonon, A., Lepage, P., Karita, E. et al. (1994) An assessment of Lyman, W.D. (1993) Perinatal AIDS: Drugs of abuse and transpla-
the timing of mother-to-child transmission of human immunode-
cental infection. Advances in Experimental Medicine and Biology 335:
ficiency virus Type 1 by means of polymerase chain reaction. Journal of Acquired Immune Deficiency Syndromes 7:952-57. Maiques, V., Garcia-Tejedor, A., Perales, A., Navarro, C. (1999) Smith, M.M. and Kuhn, L. (2000) Exclusive breast-feeding: Does it
Intrapartum fetal invasive procedures and perinatal transmission
have the potential to reduce breast- feeding transmission of HIV-
of HIV. European Journal of Obstetrics, Gynecology, and Reproductive
1? Nutritional Review 58(11):333-40. Biology 87:63-7. UNAIDS/WHO. (2002) AIDS Epidemic Update. Mandelbrot, L., Mayaux, M.J., Bongain, A. et al. (1996) Obstetric
(UNAIDS/02.58E). Geneva: Joint United Nations Programme on
factors and mother-to-child transmission of human immunodefi-
HIV/AIDS (UNAIDS) & the World Health Organization (WHO):
ciency virus type 1: The French perinatal cohorts. SEROGEST
http://www.unaids.org/worldaidsday/2002/press/update/epiup-
French Pediatric HIV Infection Study Group. American Journal ofObstetrics and Gynecology 175:661-7. UNICEF. (2003) UK Baby Friendly Initiative. Baby friendly hospi- Miotti, P.G., Taha, T.E., Kumwenda, N.I. et al. (1998) HIV trans- 138 Breast feeding and HIV transmission
JOURNAL OF neonatal NURSING VOLUME 9 ISSUE 4 2003
U.S. Agency for International Development, United Nations CBE for TVU Professor Children’s Fund, Joint United Nations Programme on HIV/AIDS. (2002) Children on the Brink 2002: A Joint Report on Orphan
Congratulations to one of our authors, Robert Pratt,
Estimates and Program Strategies. Washington DC; TvTAssociates/The Synergy Project.
Professor of Nursing and Director of the Richard
http://www.synergyaids.com/documents/COB2002.pdf
Internet resources
Valley University’sFaculty of Health and
• Anderson JR (ed.). A Guide to the Clinical Care of Women
with HIV 2001 ed. U.S. Department of Health and Human
Services, Health Resources and Services Administration,
HIV/AIDS Bureau. This excellent practical text
comprehensively describes the care and treatment of HIV-
infected women is available free (online, CD and hard copy
available.) and is regularly updated. Hard copy can be
obtained free of charge by contacting: Womencare,
Parklawn Bldg., Rm 11A-33, 5600 Fishers Lane, Rockville,
Maryland 20857, USA; Fax: +1-301-443-0791; or e-mail:
• Questions and Answers on MTCT are available from the
Professor Pratt has been a prominent and influential
figure developing care strategies for persons with
http://www.unaids.org/publications/documents/mtct/qaw
HIV disease since the beginning of the global
pandemic. During the last five years, he and his
• The Baby Friendly Initiative is a global programme of
group have developed a series of national
UNICEF and the World Health Organization which works
evidence-based guidelines for preventing
with the health services to improve practice so that parents
healthcare-associated infections on behalf of the
are enabled and supported to make informed choices about
Department of Health and the National Institute
how they feed and care for their babies. A Photographic Memory
The Child Bereavement Trust has recently produced a booklet entitled “A photographic memory”, which isdesigned as guidance for professionals responsible for offering parents photographs at the time of their baby’sdeath. As the booklet states “A picture paints a thousand words” and the guide encourages professionalscaring for parents whose baby is dying or has died, to think about the importance of photographs as part ofthe care offered to families.
The content of the booklet is based on what bereaved parents have appreciated about the photographs taken byprofessionals when their baby died. Parents share their precious photographs and feelings about their children.
The value of the booklet is in the way it sensitively demonstrateshow to take photographs of a dead baby that parents will treasure. For example photographs of tiny, perfect little hands or feet; a pictureof a little boy holding his dead sister; a photograph of a dead twinbeside her living sibling.
At the back of the booklet practical information is given includingusing polaroid and digital cameras, as well as the use of black andwhite photography. Copies of the booklet have already been distributed free of charge to each maternity and neonatal unit in the UK and further copies are available for purchase from The Child Bereavement Trust at a cost of £7.50 or 4 copies for £25. Contact CBT on [email protected] or 0845 357 1000.
JOURNAL OF neonatal NURSING VOLUME 9 ISSUE 4 2003
Breast feeding and HIV transmission 139
Utilisation des anti-sécrétoires chez les enfants opérés d’une atrésie de l’œsophage Frédéric Gottrand, Unité de Gastro-entérologie, Hépatologie et Nutrition et Centre de référence des affections congénitales et malformatives de l’œsophage, Clinique de Pédiatrie, Hôpital Jeanne de Flandre et Faculté de Médecine, Université Lille2, Lille. Mâchouille : Qu’est-c
Erdheim-Chester DiseaseA Case Study and Literature ReviewDiagnosis and treatment of patients who present with respiratorycompromise are challenging. What happens when these patients donot respond to your intervention, and their condition declines rapidly?Having a variety of differential diagnoses is key. An addition to yourdifferential list can include a rare disorder of nonYLangerhans cell
 Breast feeding and HIV transmission:
Breast feeding and HIV transmission: 
 U.S. Agency for International Development, United Nations
U.S. Agency for International Development, United Nations