Safety of fluticasone propionate cream 0.05% for the treatment of severe and extensive atopic dermatitis in children as young as 3 months
S. F. Friedlander, MD,a A. A. Hebert, MD,b and D. B. Allen, MD,c for the Fluticasone Pediatrics
Safety Study Group* San Diego, California, Houston, Texas, and Madison, WisconsinBackground: Topical corticosteroids are useful for the treatment of pediatric dermatoses. However, concerns regarding possible systemic and topical toxicities have limited the use of moderate-potency corticosteroids in children. Objective: Our purpose was to characterize the safety of fluticasone propionate cream in children. Methods: Children between 3 months and 5 years 11 months (n = 32) and 3 up to 6 years of age (n = 19) with moderate to severe atopic dermatitis (≥ 35% body surface area; mean body surface area treated, 64%) were treated with fluticasone propionate cream, 0.05% twice daily for 3 to 4 weeks. Serum cortisol response, fluticasone levels, skin changes, and adverse events were analyzed. Results: Mean cortisol levels were similar at baseline (13.76 ± 6.94 µg/dL prestimulation and 30.53 ± 7.23
µg/dL poststimulation) and at end of treatment (12.32 ± 6.92 µg/dL prestimulation and 28.84 ± 7.16 µg/dLpoststimulation). Only 2 of 43 children had end-treatment poststimulation values less than 18.0 µg/dL. Nosignificant adverse cutaneous effects were noted. Conclusion: Fluticasone propionate cream 0.05% appears to be safe for the treatment of severe eczema for up to 4 weeks in children 3 months of age and older. (J Am Acad Dermatol 2002;46:387-93.)
Atopic dermatitis affects approximately 5% to
20% of all children by 11 years of age,1 making
it the most common skin disease of child-
hood.2 Because of its chronic, recurrent nature, this
form of eczema can have a considerable impact on
the quality of life of patients and their families,
including adverse effects on sleep patterns, behavior,
family relationships, and financial stability.3 Topical
corticosteroids are commonly used to treat eczema.4
HPLC: high-pressure liquid chromatography
From the Department of Pediatrics and Medicine (Dermatology),
University of California, San Diego School of Medicine and
Children’s Hospitala; the Department of Dermatology, Universityof Texas Medical School, Houstonb; and the Department ofPediatrics, University of Wisconsin, Madison.c
Their misuse, however, may lead to skin thinning
and systemic complications such as reversible hypo-
Accepted for publication April 30, 2001.
thalamic-pituitary-adrenal (HPA) axis suppression.
Reprint requests: Sheila Fallon Friedlander, MD, Department of
Pediatrics and Medicine (Dermatology), University of California,
The occurrence of HPA axis suppression is of partic-
San Diego School of Medicine and Children’s Hospital, San
ular concern in children because of the potential for
Diego, 3030 Children’s Way, Suite 408, San Diego, CA 92123.
increased absorption caused by a higher ratio of skin
*A complete list of the members of the Fluticasone Pediatrics
Safety Group appears at the end of the article.
Topical formulations of fluticasone propionate
Copyright 2002 by the American Academy of Dermatology, Inc. 0190-9622/2002/$35.00 + 0
16/1/118337
(Cutivate, Glaxo Wellcome, Research Triangle Park,
NC), a corticosteroid,5 are indicated for the relief of
388 Friedlander, Hebert, and Allen
the inflammatory and pruritic manifestations of cor-
cant disease other than the study disease; any gross
ticosteroid-responsive dermatoses. Both the cream
physical impairment that would affect the outcome
and ointment formulations have shown minimal
of or interfere with participation in the trial; any
effects on HPA axis function in adults, as determined
unstable concomitant disease other than the condi-
by measuring morning serum or plasma cortisol con-
tion to be treated in the study; and known hypersen-
centrations.6-9 Any fluticasone propionate that is
sitivity to fluticasone propionate, its cream vehicle, or
absorbed systemically is rapidly metabolized by the
cosyntropin (Cortrosyn, Organon Inc, West Orange,
liver. The major metabolite of fluticasone propionate
NJ). Use or anticipated use of the following therapies
has no significant anti-inflammatory activity or gluco-
also resulted in exclusion from the study: topical or
corticoid activity, contributing to its low potential for
inhaled corticosteroids within 1 week of study entry;
HPA axis suppression.10-12 These unique pharmaco-
long-term therapy (>4 weeks continuously) such as
logic characteristics suggest that fluticasone propi-
cyclosporine, methotrexate, psoralen and ultraviolet
onate may be appropriate for use in pediatric
light (PUVA), or topical products for skin lesions
patients with extensive eczema in whom more
within 4 weeks; systemic corticosteroids within 6
potent corticosteroids are needed to suppress flares,
months; systemic retinoids; or any other topical or
but for whom HPA axis suppression is of concern.
systemic therapy for the study disease other than
Although the adrenal response to stimulation
bland emollients, such as moisturizers, in untreated
with cosyntropin (Cortrosyn; CST) has been tested
areas, with the exception of therapies known to have
in children after treatment with topical mometasone
no effect on cortisol values and HPA axis function.
furoate,13 no study in children has assessed the
Patients who had engaged in certain recent activities
adrenal response to stimulation with cosyntropin
(eg, the use of tanning booths, sunbathing, or UV
after extensive treatment with topical fluticasone
light treatments) or who had potentially interfering
propionate. This information is important, given the
personality characteristics or habits (subject or par-
recurrent nature of the disease and the need for safe,
ent/guardian) during the study were also excluded.
effective therapies for severe eczema in children.
Participation in another investigational drug study
Thus the purpose of the present study was to evalu-
within 4 weeks before the start of the study was not
ate the effects of fluticasone propionate cream 0.05%
on HPA axis function using CST testing and to evalu-ate its effect on other safety variables in pediatric
Study design
patients with moderate to severe eczema.
This phase IV open-label safety study was con-
ducted at 10 centers in the United States. This study
MATERIALS AND METHODS
was approved by the Institutional Review Board at
Subjects
each center. Subjects were screened up to 6 days
Pediatric patients between the ages of 3 months
before baseline. After the baseline visit (day 1), visits
and 5 years 11 months with extensive moderate to
occurred weekly for 3 to 4 weeks. At baseline and at
severe psoriasis or eczema (excluding acute self-
the end of treatment visit, HPA axis function was
limiting eczema) were considered for enrollment.
determined by the response to CST, and blood was
Their condition must have been stable or worsening
collected for clinical laboratory tests (serum chem-
and must have involved at least 35% of body surface
istry, hematology, and assay of plasma fluticasone
area (BSA) (not counting lesions in the diaper area
propionate concentrations). Proactive monitoring
for subjects who wore diapers; also excluding lesions
for adverse events, signs of skin atrophy, and skin
on the eyelids, in the perioral area, in the nostrils,
pigmentation changes was conducted weekly.
and in areas where corticosteroid treatment was con-
Subjects who had abnormal CST results, other labo-
traindicated). The total severity score was required to
ratory abnormalities, or adverse events that required
equal at least 6.0 for any 3 of 8 potential signs and
follow-up were seen 1 or 2 weeks after the end of
symptoms (erythema, pruritus, papulation, indura-
tion, oozing/crusting, scaling, excoriation, lichenifica-
Fluticasone propionate cream 0.05% was applied
tion), for which each sign/symptom was rated on a
twice daily to all lesions, including facial lesions, but
scale of 0.0 (absent) to 3.0 (severe).14 BSA was esti-
not including those in the diaper area, eyelids, peri-
mated using the “rule of nines.”15 Subjects were strat-
oral area, nostrils, and areas in which corticosteroid
ified into 2 age groups: (1) 3 months to less than 3
treatment was contraindicated, such as those show-
years (younger group) and (2) 3 years to less than 6
ing signs of atrophy. The amount necessary to cover
years (older group). Written informed consent was
the lesions was based on the fingertip unit, a ribbon
obtained from the parent or guardian of all patients
of cream the length of the tip of the guardian’s index
before study entry. Exclusion criteria included signifi-
finger (second phalanx).16 The investigator was
Friedlander, Hebert, and Allen 389
expected to estimate the amount of cream that
phy (HPLC) only in subjects 2 years of age and older,
would make up the guardian’s fingertip unit and to
to minimize the amount of blood drawn from chil-
demonstrate to the guardian how much cream to
dren younger than 2 years of age. For poststimula-
apply based on the extent of BSA to be treated.
tion CST results, the lower limit of normal for serum
Maximum drug exposure conditions were main-
cortisol level was 18 µg/dL for FPIA and 14.5 µg/dL
tained by treating twice daily (fluticasone propionate
for HPLC. The minimal value detectable of cortisol
0.05% is currently approved for once- or twice-daily
was 1.0 µg/dL for the FPIA method and 0.5 µg/dL for
application in the treatment of atopic dermatitis)
and continuing treatment for 1 week after subjects’
The primary indicator of a normal adrenal
lesional areas were assessed as cleared or for a max-
response was defined as a poststimulation cortisol
imum of 4 weeks. Clearing was defined as loss of
peak value of more than 18.0 µg/dL by FPIA. The
signs or symptoms of disease and no residual ery-
FPIA was chosen as the primary indicator of normal
thema. A minimum of 35% BSA was treated regard-
adrenal response because FPIA results were avail-
less of healing for 3 to 4 weeks to maintain adequate
able to investigator sites within 24 hours of receipt.
conditions for testing the effects of systemic absorp-
In addition, given the need to restrict HPLC analy-
tion of the drug and evaluation of local side effects.
ses to the older age group because of blood volume
At each weekly visit, signs and symptoms of disease
concerns for the younger group, only FPIA values
(eg, erythema, pruritus, papulation, induration, ooz-
were available for all subjects. Of note is the corre-
ing/crusting, scaling, excoriation, and lichenification)
lation (>0.577 and >0.85 at 1 of 4 and 3 of 4 time
were evaluated to monitor compliance and to assess
points, respectively) between the cortisol data gen-
the extent of exposure to study drug. Healed skin
erated by the FPIA assay and HPLC assay (P < .001)
would be expected to absorb less study drug than
at each time point as determined by the Spearman
diseased skin, although recently cleared lesional
correlation coefficient. Thus, had there been both
areas continue to exhibit less than normal barrier
FPIA and HPLC cortisol data for all subjects, data
function.17 In an effort to monitor compliance, all
from either assay could have been used to evaluate
returned medication tubes were weighed.
To assess consistency and to evaluate marginal
Safety assessments
responses, other criteria stated in the product infor-
Safety parameters included adrenal response to
mation for CST were also examined, specifically, a
CST, signs of skin atrophy and pigmentation changes,
prestimulation to poststimulation increase in corti-
changes in hematology and serum chemistries, and
sol of approximately 2-fold (provided the prestimu-
occurrence of adverse events. Plasma fluticasone val-
lation value did not exceed the normal range) or an
ues were measured only in subjects 2 years of age and
increase of 7 µg/dL or more. CST results were also
older because of the limited amount of blood that
reviewed by a pediatric endocrinologist (D. B. A.).
could be drawn from younger subjects. A fasting
Skin thinning and other signs associated with
blood sample was obtained for analysis of serum cor-
atrophy were assessed by 2× magnification and
tisol and clinical laboratory tests. Covance Central
included telangiectasia, loss of elasticity, purpura,
Laboratory Services, Inc, Princeton, New Jersey, per-
dusky erythema, and striae. These signs were scored
formed all serum chemistries, hematology values, and
according to severity. Any pigmentation change not
considered to represent a normal healing process
For the CST analyses, the baseline blood draw
was reported as an adverse event. Treated skin was
occurred on the morning of day 1, and the end-
assessed by the investigator at each visit. Baseline
treatment blood draw occurred on day 22 or 29.
and end-of-treatment analyses of serum chemistries
Prestimulation blood samples were obtained at 8 AM.
were performed for concentrations of alkaline phos-
CST was administered intravenously immediately
phatase, lactate dehydrogenase (LDH), aspartate
after prestimulation blood samples had been
aminotransferase (AST), alanine aminotransferase
obtained. The dose of CST was 0.125 mg for subjects
(ALT), glucose, total protein, albumin, sodium,
in the younger group and 0.25 mg for subjects in the
potassium chloride, total carbon dioxide, phospho-
older group. A poststimulation blood sample was
rus, uric acid, blood urea nitrogen (BUN), creatinine,
obtained 30 minutes after the injection of CST.
calcium, and total bilirubin. Hematology assessment
Subjects were offered food or drink after the admin-
included white blood cell (WBC) count and differen-
istration of CST and before collection of the post-
tial, red blood cell (RBC) count and morphology,
stimulation sample. Serum cortisol was assayed by
platelet count, hematocrit, and hemoglobin. Adverse
fluorescence-polarization immunoassay (FPIA) in all
events were recorded as to nature, severity, and rela-
subjects and by high-pressure liquid chromatogra-
390 Friedlander, Hebert, and Allen Table I. Summary of baseline demographic and Table II. Summary of baseline dermatologic groups (total) groups (total)
*Age and weight were determined at the screening visit ratherthan at baseline.
tion and poststimulation samples) available from 43of the 51 subjects comprising the intent-to-treat pop-ulation. CST results are presented for all subjects (n
Plasma fluticasone concentrations were deter-
= 46 prestimulation, n = 43 poststimulation) with
mined by automated solid-phase extraction using a
end-of-treatment CST (at day 22, day 29, or at the
Zymark 96-well system (Zymark Corp, Hopkinton,
end of treatment for subjects who discontinued,
Mass). The extracts were analyzed by HPLC with tan-
regardless of treatment duration). Correlations using
dem mass spectrometric detection, using a reverse-
the Spearman correlation coefficient were also
phase column. The calibration range was 50 to 1520
assessed between CST results and age, between the
pg/mL from 0.5 mL of plasma, with a limit of detec-
ratio of the amount of drug used to the BSA affected,
and the ratio of the amount of drug used to the end-of-treatment poststimulation cortisol results. Statistical analysis
Data, including demographics, adverse events,
and occurrence of atrophy and associated signs,
Study population
were summarized using the intent-to-treat popula-
Fifty-one children, 32 in the younger group (age
tion consisting of the 51 enrolled subjects. The CST
3-35 months; median, 20 months) and 19 in the
data presented are based on complete blood sample
older group (age 36-70 months; median, 50 months)
sets (baseline and end of treatment for prestimula-
were enrolled, all of whom had atopic dermatitis. In
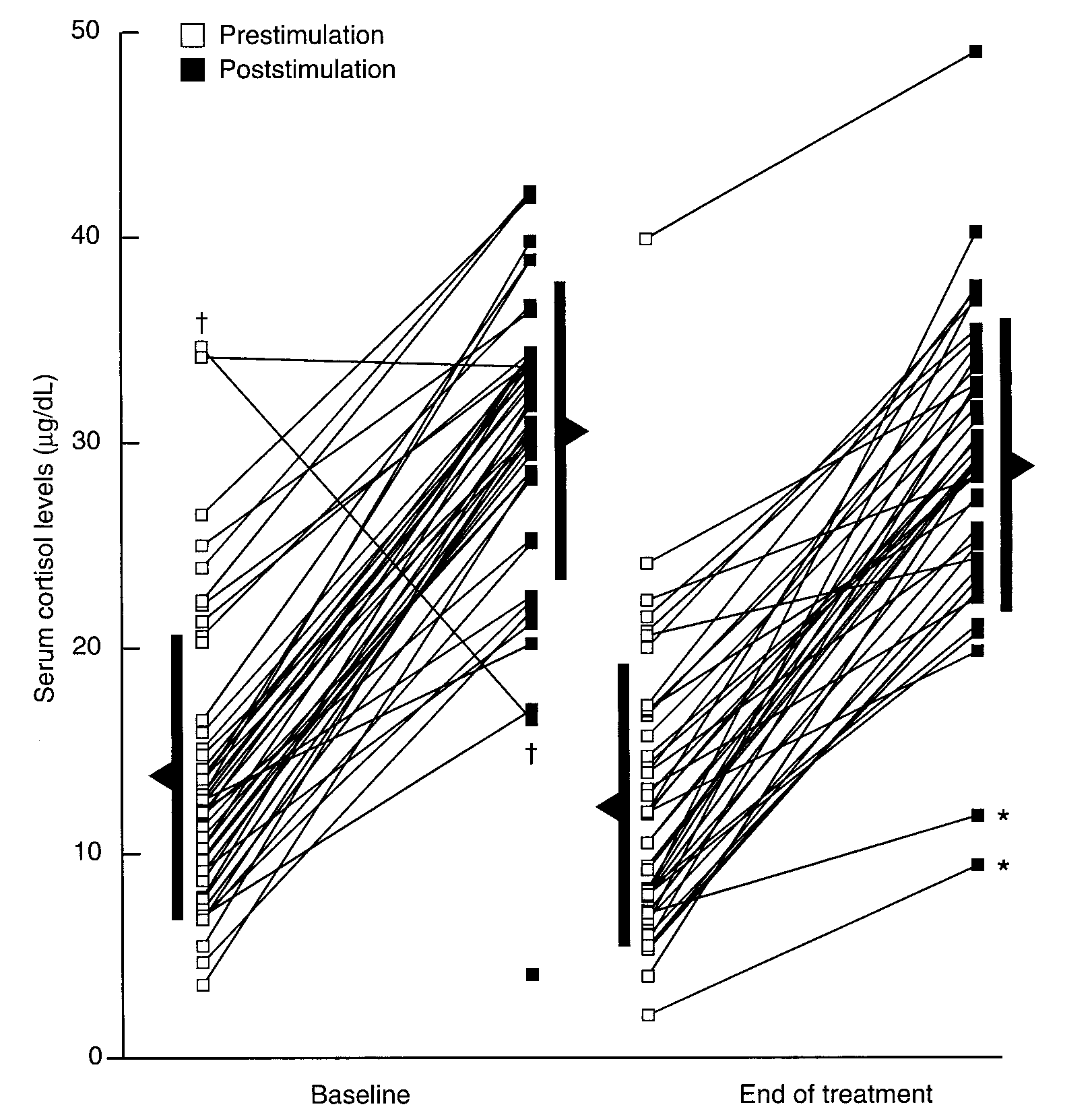
Friedlander, Hebert, and Allen 391 Fig 1. Serum cortisol levels for all subjects at baseline (n = 49 prestimulation, n = 47 post- stimulation) and end of treatment (n = 46 prestimulation, n = 43 poststimulation) with fluti- casone propionate (for 22-30 days) before and after 30-minute CST stimulation as assessed by FPIA. Heavy black bars indicate mean ± 1 standard deviation. Asterisk, Children considered to have HPA suppression; dagger, apparent laboratory error.
the younger group, 8 children were younger than 12
group and 7.7 g (53.9 g/wk) in the older group. At
months (4 were 3-6 months and 4 were 7-11
baseline, cutaneous atrophy was not reported for
months). Demographic and baseline dermatologic
any child and only one child had telangiectasia
characteristics are shown in Tables I and II, respec-
(mild). Eight younger children (25%) and 3 older
tively. Subjects were evenly distributed between the
children (16%) had abnormal pigmentation.
sexes, and the majority were Caucasian (39%). The
Five children in the older group discontinued pre-
remaining children were African American (29%),
maturely, 2 children before treatment because of
Asian (16%), American Hispanic (8%), or other (8%).
inability to draw blood, and 3 children during treat-
All children had a diagnosis of eczema at baseline,
ment because of loss to follow-up (1 patient), inade-
considered to be worsening in 76% of patients and
quate disease severity at baseline (1), and an abnor-
stable in the remainder. The mean duration of the
mal baseline CST (1). The 3 children who were dis-
current eczematous episodes at this time was 45.7
continued during treatment were treated for less
weeks for the younger group and 107.7 weeks for
the older group. The mean baseline BSA treated was62.3%, with a range of 35% to 94% in the younger
Safety results
group and 67.2%, with a range of 36% to 95%, in the
Adrenal responsiveness. The serum cortisol
older group. The mean baseline BSA treated was
levels are presented in Fig 1. No meaningful differ-
64% for all subjects. The average amount of drug
ences were seen in mean prestimulation and post-
used per day was 3.8 g (26.6 g/wk) in the younger
stimulation cortisol levels between baseline and the
392 Friedlander, Hebert, and Allen
end of treatment. Mean cortisol levels at baseline
pression using 18 µg/dL as the lower limit of normal.
were 13.76 µg/dL (standard deviation [SD], 6.94
However, the HPLC value was actually higher than
µg/dL) before stimulation and 30.53 µg/dL (SD, 7.23
14.5 µg/dL, the lower limit of normal for the HPLC
µg/dL) after stimulation, and at the end of treatment
assay. In addition, the FPIA prestimulation and post-
these values were 12.32 µg/dL (SD, 6.92 µg/dL)
stimulation cortisol levels were normal, 13.1 µg/dL
before stimulation and 28.84 µg/dL (SD, 7.16 µg/dL)
and 22.4 µg/dL, respectively, and the follow-up FPIA
after stimulation (Fig 1). Furthermore, the mean dif-
and HPLC prestimulation and poststimulation corti-
ferences between baseline and end of treatment in
sol levels were also normal, so this child ultimately
prestimulation and poststimulation cortisol values
were small (–1.78 µg/dL, P = .1734; –2.49 µg/dL, P =
Very little correlation existed between age and
either FPIA- or HPLC-generated cortisol data (P > .1
Of the 43 children with end-of-treatment post-
at all time points; correlation coefficient [r] of age
stimulation cortisol values, only 2 (4.7%) had values
with baseline and end of treatment for FPIA data,
that did not exceed 18.0 µg/dL. The baseline values
–0.20 and –0.17, respectively; correlation coefficient
of these 2 subjects were 22.1µg/dL (prestimulation),
[r] with baseline and end of treatment for HPLC
33.9 µg/dL (poststimulation) and 10.8 µg/dL (pres-
data, –0.16 and –0.19, respectively). There was some
timulation), 28.6 µg/dL (poststimulation). The end-
correlation between the ratio of the amount of drug
of-treatment values were 7.1 µg/dL (prestimulation),
used to BSA affected and end-of-treatment poststim-
11.8 µg/dL (poststimulation) and 2.1 µg/dL (prestim-
ulation cortisol results (r = –0.40; P = .02).
ulation), 9.4 µg/dL (poststimulation), respectively. Relationship of plasma fluticasone concen-
These 2 children, 1 from each age group, were con-
trations to cortisol levels. No child had measur-
sidered to exhibit HPA axis suppression. One of
able fluticasone values at baseline. Six of 25 children
these children (age 5 years, 101 cm, 18.1 kg) had
(24%) who had plasma samples taken at end of treat-
normal CST at follow-up, 12 days after the last dose
ment for measurement of fluticasone had measur-
of study medication (2.1 µg/dL, prestimulation and
able concentrations of the drug, 3 in each age group.
19.8 µg/dL, poststimulation). This child had 95% BSA
The mean fluticasone plasma concentrations were
affected and was treated for a duration of 4 weeks
112.1 pg/mL (range, 59-155 pg/mL) in the younger
(561.0 g of medication used). The other child (age 2
group, 163.1 pg/mL (range, 109-264 pg/mL) in the
years, 91 cm, 13.1 kg), who had 35% BSA affected
older group, and 137.6 pg/mL (range, 59-264 pg/mL)
and was treated for a duration of 5 weeks (176.5 g of
medication used), was lost to follow-up. The 5-year-
There were insufficient data to analyze relation-
old used more medication than the others in this age
ships between plasma fluticasone concentrations
group (mean, 209.1 g), and the 2-year-old used more
and cortisol levels. However, detectable plasma fluti-
than the mean amount used in his age group (96.7
casone concentrations were present in only 1 of the
g) but less than the maximum amount of 355.7 g.
2 children considered to have adrenal suppression
These 2 subjects are shown in Fig 1 as the 2 points
(plasma fluticasone concentration, 116.5 pg/mL
(indicated with an asterisk) with the lowest end-of-
(0.01165 µg/dL), end-of-treatment poststimulation
cortisol value, 11.8 µg/dL) and in only 1 of the 2 chil-
Two other children in the younger group had end-
dren in whom there was the suggestion of evolving
of-treatment poststimulation cortisol levels indicat-
adrenal suppression (plasma fluticasone concentra-
ing adrenal suppression by HPLC but not by FPIA.
tion, 122.0 pg/mL, end-of-treatment poststimulation
However, since the FPIA level trended low in one
cortisol value, 19.8 µg/dL). The child with the high-
subject and did not show an increase of 7 µg/dL or
est plasma fluticasone concentration (264 pg/mL)
more in the other subject, it was noted that this pos-
did not have adrenal suppression (end-of-treatment
sibly suggested evolving adrenal suppression in
poststimulation cortisol value, 23.3 µg/dL).
these 2 children. Of note is that the protocol exclu-
Adverse events involving the skin. Twenty-five
sion criteria were violated by the use of long-term
children (50%) had 39 adverse events, most fre-
corticosteroid treatment in one child within 4 weeks
quently fever and cold symptoms. Only 7 drug-
of the study. Both of these children had a normal
related adverse events were reported in 5 children.
One event occurred in 1 subject in the younger
Finally, one investigator reported mild adrenal
group and 6 events occurred in 4 subjects in the
suppression in a child in the younger group. Owing
older group (1 event in 3 subjects and 3 events in 1
to a laboratory error, this younger child’s cortisol
subject). These 7 events were local events and
level was assessed by both FPIA and HPLC. The
included 1 event each of burning and urticaria (both
HPLC value, 17.2 µg/dL, was thought to suggest sup-
resolved without action the day they were reported),
Friedlander, Hebert, and Allen 393
1 event of erythematous rash (resolved with discon-
Specifically, it has a low potential for HPA axis sup-
tinuation of the practice of applying drug to moist
pression and for induction of atrophogenic effects,
skin after bathing), and 3 events of telangiectasia (2
even after extensive application (mean baseline BSA
facial and 1 nonfacial). The facial telangiectasia in
both subjects may have been a preexisting conditionunmasked with resolution of the eczema. Both cases
The Fluticasone in Pediatrics Safety Study Group con-
of facial telangiectasia were resolved within 1 month
sists of the following investigators: P. J. Honig, A. Paller, D.
after cessation of study drug. In addition, 1 subject
J. Hogan, A. W. Lucky, J. Hanifin, A. Hebert, E. Siegfried, S.
with facial and nonfacial telangiectasia also had mild
A. Raimer, S. Fallon Friedlander, D. B. Allen DB, and Y. H.
dusky erythema, which resolved within 1 month
after study drug cessation. Whether or not the non-
REFERENCES
facial telangiectasia resolved is unknown.
1. Williams HC. On the definition and epidemiology of atopic der-
No child had pigmentation changes assessed as
matitis. Dermatol Clin 1995;13:649-57.
treatment related, and fewer patients had abnormal
2. Kim HJ, Honig PJ. Atopic dermatitis. Curr Opin Pediatr 1998;10:
pigmentation during and after treatment (11%-14%)
3. Lawson V, Lewis-Jones MS, Reid P, Owens RG, Finlay AY. Family
impact of childhood atopic eczema [abstract]. Br J Dermatol
There were no deaths, serious adverse events, or
discontinuations caused by adverse events. There
4. Friedman PS. Allergy and the skin: II–contact and atopic
were no drug-related, clinically significant shifts in
serum chemistry results or hematology values.
5. Högger P, Rohdewald P. Binding kinetics of fluticasone propi-
onate to the human glucocorticoid receptor. Steroids 1994;59:597-602. DISCUSSION
6. Young MMR, Sohail S, Harding SM. A comparison of the sys-
This phase IV open-label study demonstrated that
temic absorption of fluticasone propionate and betametha-
fluticasone propionate cream 0.05% applied twice
sone valerate after topical application of cream formulations
daily for 3 to 4 weeks over a large BSA (mean, 64%)
[abstract]. Br J Dermatol 1994;131(Suppl 44):35-6.
has a low potential to suppress HPA axis function in
7. Tschen E, Bucko AD. Assessment of HPA-axis suppression with
fluticasone cream 0.05% in patients with extensive psoriasis or
children as young as 3 months of age who have mod-
eczema. Clin Drug Invest 1968;16:111-6.
erate to severe eczema. Infrequently, HPA axis sup-
8. Cornell R. Fluticasone propionate ointment, 0.005%: its lack of
pression can occur, and therefore periodic monitor-
suppression on the hypothalamic-pituitary-adrenal axis when
ing is appropriate in high-risk patients. Monitoring
used for treatment of psoriasis or eczema. Presented as a poster
may be carried out by CST, morning plasma cortisol
abstract at the 54th Annual Meeting of the American Academyof Dermatology, Washington, DC, Feb 10-15,1996.
levels, and urine-free cortisol tests. If HPA axis sup-
9. Juhlin L. Comparison of fluticasone propionate cream, 0.05%
pression occurs, withdrawal of the drug, reduction
and hydrocortisone-17-butyrate cream, 0.1% in the treatment
of the frequency of application, or substitution of a
of eczema. Cutis 1996;57(Suppl):51-6.
less potent steroid should be considered. Recovery
10. Phillipps GH. Structure-activity relationships of topically active
of HPA axis function is generally rapid after discon-
steroids: the selection of fluticasone propionate. Respir Med1990;84(Suppl A):19-23.
tinuation of topical corticosteroids. Rarely, signs and
11. Johnson M. Fluticasone propionate: safety profile. Cutis 1996;
symptoms of glucocorticoid insufficiency may occur,
requiring supplemental systemic corticosteroids. In
12. Spencer CM, Wiseman LR. Topical fluticasone propionate: a
this study, effects on the HPA axis were rapidly
review of its pharmacological properties and therapeutic use in
reversible in susceptible patients. There was no
the treatment of dermatological disorders. BioDrugs 1997;7:318-34.
apparent relationship between plasma concentra-
13. Hanifin J.The role of topical steroids in the treatment of allergic
tion and the development of adrenal suppression.
skin disease. Symposium Highlights, 12th Regional Conference
Indeed, as noted earlier, the child with the highest
of Dermatology, Pattaya, Thailand, May 11, 1996, Conference
plasma fluticasone concentration did not have
14. Hanifin JM. Standardized grading of subjects for clinical
research studies in atopic dermatitis: workshop report. Acta
In addition, the results of this study suggest that
fluticasone propionate cream 0.05% has a low poten-
15. Knaysi GA, Crikelair GF, Cosman B. The rule of nines: its history
tial for atrophogenic effects, even after extensive
and accuracy. Plast Reconstr Surg 1968;41:560-3.
treatment with large quantities of the drug.
16. Long CC, Mills CM, Finlay AY. A practical guide to topical thera-
Fluticasone propionate cream 0.05% has an excel-
py in children. Br J Dermatol 1998;138:293-6.
17. Stoughton RB, Cornell RC. Corticosteroids. In: Fitzpatrick TB,
lent safety profile when used in the treatment of
Eisen AZ,Wolff K, Freedberg IM, Austen KF, editors. Dermatology
moderate to severe atopic dermatitis for up to 4
in general medicine. 4th ed. New York: McGraw-Hill; 1993. p.
weeks in children 3 months of age and older.
Newsletter –Fall Edition 2004 Richard Cramer, Pharm D Kimberly Chandler, Pharm D Bob Delaney, M.S. Dan Gillis, Pharm D Steve McDonald, Pharm D Update on Treatment of Parkinson’s Disease Christal Smith Taylor, PharmD Candidate Samford University McWhorter School of Pharmacy Since James Parkinson’s publication on The Shaking Palsy in 1817, the treatment o
The question of gender identity in the modern Hungarian female The previously neglected areas of cultural arts and the arts dealing with the social role of the genders may have become the pillars of thinking at the end of the 20th century in the human sciences because civilisation had reached one of its deepest crises as a result of the elimination of the thousands of years long system of v
 Friedlander, Hebert, and Allen 391
Friedlander, Hebert, and Allen 391