Neurourology
Is tolterodine as effective as oxybutynin in overactive bladdercaused by spinal cord injury?
ELENA ANDRETTA1, BRUNO BONADIMANI2, MAURO PASTORELLO3, ENRICO COSSARO1,GIORGIO ARTUSO1
1Department of Urology, General Hospital Dolo (Venice), Italy2Faculty of Pharmacy, University Padua, Italy3Department of Urology General Hospital of Negrar, Verona, Italy Abstract: Abstract: In neuro-urological practice the immediate release oxybutynin - the extended release one has become available in Italy on-ly in 2010 - is usually considered more effective than the immediate release tolterodine in the treatment of overactive bladder caused by spi-nal cord injury. But in literature there is no a clear evidence, mainly for lack of papers on this topic. We reviewed records of patients with spinal cord injury from January 1996 and June 2009. We found 16 patients (11 males and 5 females,mean age 43.5 years, range 22-67) that switched the antimuscarinic treatment from one drug to the other one having been checked by vide-ourodynamic examinations during the assumption of each drug. The drugs were assumed at the usual dosages (tolterodine 2 mg twice a dayand oxybutinin 5 mg twice or three times a day with an average of 12.5 mg). The efficacy of the antimuscarinics has been estimated clinical-ly, based on the micturition diaries, and instrumentally, based on the modifications of the urodynamic parameters. Oxybutynin has resultedmore effective than tolterodine at the recommended dosage for 75% of patients with detrusor-sphincter dyssinergy caused by sovrasacral spi-nal cord injury. Videourodynamic studies showed an increase of cystometric bladder capacity and a decrease of detrusor pressure in compa-rison with tolterodine. The statistical comparison between the two averages relative to maximal detrusor pressure and bladder cystometric ca-pacity determined by using the “Student test for data joined to a tail” has turned out meaningful for p<0,01. Key words: Antimuscarinics; Neurogenic bladder; Spinal cord injury; Urodynamics
placed by OX, as TL wasn’t effective in the cure of the
Many neurourologists consider oxybutynin (OX) more
urinary incontinence. The drugs were assumed at the usual
effective than tolterodine (TL) in the treatment of the over-
dosages: TL 2 mg twice a day and OX at the dose of 5 mg
active bladder caused by the sovrasacral spinal cord injury
twice or three times a day (average of 12.5 mg/die).
(SCI) in the picture of the detrusor-sphincter dyssinergy
Thirteen patients voided by self-CIC while 3 women, at
(DESD). In DESD the antimuscarinics are usually used to
the beginning treated with TL, voided by reflex micturi-
abolish detrusor contractions in order to permit voidings by
tions. The videourodynamic examination was carried out at
clean intermittent catheterism (CIC). However, in literature
least 2 months after the assumption of each drug (range 2-
there is no a clear and well established evidence although
13 months, mean 3.8) and it was performed in the lytotom-
these drugs were mainly compared in idiopathic overactive
ic position using one double-lumen transurethral catheter 6
bladder or in a few and different types of neurogenic over-
Ch and one rectal probe. Iodinated contrast medium was in-
fused at a flow rate of body weight/4 ml/min and a Med -
In Italy the extended release OX has become available
tronic Duet system was used. Urinary sterility and regular-
only in 2010. On the other hand the immediate release OX
ity of urinary tracts by ecography were checked previously.
is still nowadays the main antimuscarinic agent used for
For all patients the micturition diaries of 4 days were avail-
neurogenic bladder as the generic drug is dispensed free of
charge by the National Health System to the SCI patients.
The effectiveness of the therapies has been estimated: a)
Therefore we reviewed the records of the SCI cases refer-
clinically, based on the micturition diaries and on the uri-
ring to our departments in order to identify the patients who
nary leakages; b) instrumentally, based on the modifica-
switched the immediate release antimuscarinic therapy –
from TL to OX or otherwise – and who underwent
A “t of Student for data joined to a tail” test was applied
videourodynamic studies during the assumption of each
to compare the different values of maximum cystometric
capacity and maximal detrusor pressure during treatmentswith OX and TL. Statistically significant difference was ac-cepted for p < 0.05.
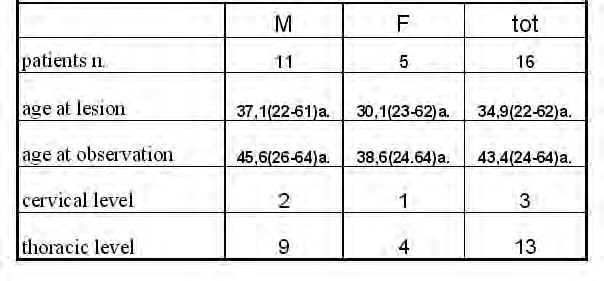
Between January 1996 and June 2009 16 patients have
met our inclusion criteria: they should have been treated in
different times with OX and TL, they should have under-
gone urodynamics during the assumption of each drug andthe urodynamic examination should have been performedat least 2 month after the beginning of the assumption ofeach antimuscarinic agent (see tab. 1).
All the patients presented DESD caused by at least a two
year stabilized sovrasacral SCI and all of them had tochange the therapy in use: 11 patients discontinued OX,and changed with TL, for comparison of side-effects (mod-erate/severe dry mouth in 10 patients and tachycardia in 1)while in 5 subjects TL assumption was interrupted, and re-
Pelviperineology 2011; 30: 10-12 http://www.pelviperineology.org
Is tolterodine as effective as oxybutynin in overactive bladder caused by spinal cord injury?
There exists only limited literature on the use of antimus-
carinics in patients with neurogenic incontinence.
In 12 patients (75%) OX improved the storage bladder
The overactive bladder caused by sovrasacral SCI is a
symptoms in comparison with TL: 9 of them complained
suitable model to compare the effects of antimuscarinic
urinary incontinence only during the therapy with TL while
drugs since the detrusor contraction is reflex in such pa-
3 patients were incontinent with both the drugs but the uri-
tients and it is not influenced by psychological inhibition.
nary leakages worsened during the treatment with TL. Also
But, on the other hand, it is really problematic to compare
the voided volumes increased during the treatment with OX
antimuscarinics in randomised or prospective trials in such
(9-46% more than with TL, with an average of 26%).
Four patients were unchanged with both the drugs and 2
OX generally causes a significantly higher incidence of
of them, complaining urinary leakages, underwent detruso-
adverse events than TL4,7,10 and this feature have been great-
ly underlined in last years. Especially the frequent dry
OX caused complete urinary retention in 2 women that
mouth induced by OX, reported in 30-60% of cases based
previously voided by reflex micturitions.
on different series, has led to find alternative drugs and TLhas been the molecule more used in 1990s, even though
few studies proved its efficacy in neurogenic overactive
All the patients showed DESD with normal compliance
and hypo-anestesia of the bladder. None showed vescico-
In a randomised study including 33% SCI patients, Van
ureteral reflux or major radiological alterations.
Kerrebroeck and all showed that TL was more effective
The average maximum cystometric capacity was 253 ±
than placebo in treating the symptoms of overactive bladder
126 ml with TL against 323 ± 111 ml observed during OX
and that the therapeutic effect was dose-dependent.1
treatment: therefore OX increased the maximum cystomet-
Later only Ethans2 compared OX and TL in 10 patients
ric capacity of 80 cc (38%) in average, respect to TL. All
with neurogenic overactive bladder – in 7 of them caused
the values are shown in fig. 1. The statistical comparison
by SCI – but in self-selected doses regimen. He reported
between the two averages executed with the test “t of
that the efficacy of TL was comparable to OX in enhancing
Student for data joined to a tail” has turned out meaningful
bladder volume, improving continence and cystometric
bladder capacity but OX presented a worse side effect pro-
The maximal detrusor pressure was reduced by OX: from
file (dry mouth). In this study larger doses of TL have been
an average of 43.5 ± 24.4 cm H2O with TL to an average
used to achieve this effect: TL twice daily at the average
of 31.2 ± 16,7 (range 0- 53 cm H2O less, mean 12.3 corre-
dose of 8 mg has been compared with OX twice daily at the
sponding to a mean percentage decrease of 19% - see fig.
2). The statistical comparison between the two averages ex-
Further Horstmann3 suggested to double TL and trospi-
ecuted with the test “t of Student for data joined to a tail”
um chloride doses in neurogenic overactive bladder not re-
has turned out meaningful for p < 0,01.
sponding to the usual dosages. Two doses of extended re-
In 4 patients (25%) urodynamic data were the same dur-
lease TL, 4 mg and 8 mg respectively, were compared and
a significant amelioration of urodynamic parameters with
In conclusion a situation of low-pressure bladder – as-
suming a cut-off for maximal detrusorial pressure < 30 cm
In the last years Cameron4 and again the group of
during cystometry – has been reached in 9 patients during
Horstman5 proposed to combine two or more antimus-
OX treatment and in 4 subjects during TL therapy.
carinics in neurogenic bladder resistant to monotherapy.
Figure 1. – Maximum cystometric capacity (MCV) for any patient in consecutively treatment with oxybutynin and tolterodine. Elena Andretta, Bruno Bonadimani, Mauro Pastorello, Enrico Cossaro, Giorgio Artuso
Figure 2. – Maximum detrusor pressure (PMax) for any patient in consecutively treatment with oxybutynin and tolterodine.
Many SCI patients referring to our neuro-urological de-
Ethans KD, Nance PW, Bard RJ, Casey AR, Schryvers OI.
partments assume OX and most of them are satisfacted. We
Efficacy and safety of tolterodine in people with neurogenic
reviewed all our records and we found a little and homoge-
detrusor overactivity. J Spinal Cord Med 2004;27:214-18
neous group of sovrasacral SCI patients who assumed in
Horstmann M, Schaefer T, Aguilar Y, Stenzl A, Sievert KD. Neurogenic bladder treatment by doubling the recommended
different times the immediate release forms of TL and OX
antimuscarinic dosage. Neurourol Urodyn 2006;25: 441-4
at usual dosages and who were checked instrumentally dur-
4. Cameron AP, Clemens JQ, Latini JM, McGuire EJ.
ing both the therapies. Even though the usual methodologi-
Combination drug therapy improves compliance of the neuro-
cal and ethical limits in studies regarding SCI patients – the
studies are mainly retrospective and based on a small
Amend B, Hennenlotter J, Schafer T, Horstmann M, Stenzl A,
number of patients – the higher efficacy of OX was ob-
Sievert KD. Effective treatment of neruogenic detrusor dys-
served in 75% of cases both clinically – disappearance of
function by combined high-dosed antimuscarinics without in-
urinary incontinence and enhancing voided volumes – than
creased side-effects. Eur Urol 2008;53:1021-8
Lee JG, Hong JY, Choo MS, Kwon HY, Chung do Y, Lee KS,
instrumentally with a mean increased of 38% as regard the
Lee JY, Lee T. Tolterodine: as effective but better tolerated
cystometric bladder capacity and a mean percentage de-
than oxybutynin in Asian patients with symptoms of overac-
crease of 19% of maximum detrusor pressure. Therefore
the usual dosage of TL shouldn’t be used in overactive
Chapple CR, Khullar V, Gabriel Z, Muston D, Bitoun CE,
bladder due to SCI except than in patients who void by re-
Weinstein D. The effects of antimuscarinic treatments in over-
flex micturitions in a safe way and in whom a reduction of
active bladder: an update of systematic review and meta-
urgency is searched (but low dosages of OX could also be
used in these rare situations). In our opinion in case of ad-
Kennelly MJ, Devoe WB. Overactive bladder: pharmacologi-
verse events caused by OX it is better to prescribe trospi-
cal treatments in the neurogenic population. Rev Urol2008;10:182-91
um chloride or detrusorial injections of botulinum toxin
Abrams P, Malone-Lee J, Jaquetin B et al. Twelve-months
treatment of overactive bladder: efficacy and tolerability oftolterodine. Drugs Aging. 2001;18:551-60
10. Jonville AP, Dutertre JP, Barbellion M. Adverse effects of oxy-
butynin chloride (Ditropan) in pediatrics. Arch Fr Pediatr1993;50:27-9
The immediate release OX is still the reference antimus-
carinic drug in SCI patients in Italy as it effectiveness is
11. Todorova A, Vonderheid-Guth B, Dimpfel W. Effects of
tolterodine, trospium chloride,and oxybutynin on the central
well-supported by daily activity and the literature.
In our experience OX has proven to be more effective
than the immediate release form of TL for 75% of SCI pa-tients with detrusor-sphincter dyssinergy.
Van Kerrebroeck PE, Amarenco G, Thuroff JW, Madersbacher
HG, Lock MT, Messelink EJ, Soler JM. Dose-ranging study of
tolterodine in patients with detrusor hyperreflexia Neurourol
Intersection forms on twisted cohomology groupsDepartment of Computational Science, Kanazawa UniversityLet h 1 , . . . , hN be linear forms in C[ x 1 , . . . , xn ]. We call the set of linearforms {h 1 , . . . , hN } a hyperplane arrangement. Put X = { ( x 1 , . . . , xn ) ∈ C n | kd log hk where λk is a given constant. Define ∇ + τ = dτ + ω ∧ τ and ∇−τ =
• Tidak selalu dapat menemukan premis yang memadai• Contoh: tidak dapat menemukan jumlah gigi di mulut kuda• Kurang disukai oleh ahli filsafat zaman kuno• Digalakkan oleh Roger Bacon, Francis Bacon, David Hume, dan lainnya• Mulai dari kasus yang cukup menuju ke generalisasi• Kelemahan: terjadi lompatan dari sebagian menjadi semua• Berdasarkan kasus membuat kesimpulan berlaku un
 Neurourology
Neurourology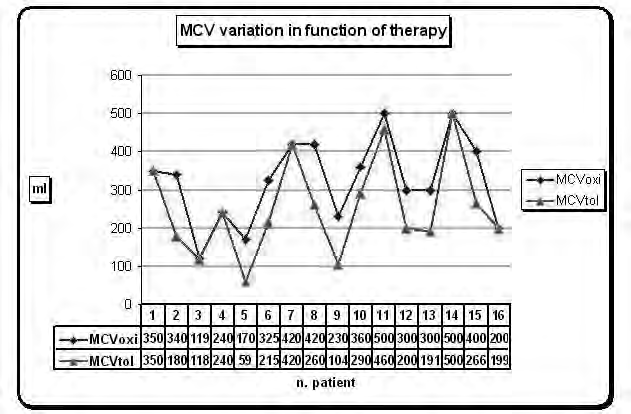 Is tolterodine as effective as oxybutynin in overactive bladder caused by spinal cord injury?
There exists only limited literature on the use of antimus-
carinics in patients with neurogenic incontinence.
In 12 patients (75%) OX improved the storage bladder
The overactive bladder caused by sovrasacral SCI is a
symptoms in comparison with TL: 9 of them complained
suitable model to compare the effects of antimuscarinic
urinary incontinence only during the therapy with TL while
drugs since the detrusor contraction is reflex in such pa-
3 patients were incontinent with both the drugs but the uri-
tients and it is not influenced by psychological inhibition.
Is tolterodine as effective as oxybutynin in overactive bladder caused by spinal cord injury?
There exists only limited literature on the use of antimus-
carinics in patients with neurogenic incontinence.
In 12 patients (75%) OX improved the storage bladder
The overactive bladder caused by sovrasacral SCI is a
symptoms in comparison with TL: 9 of them complained
suitable model to compare the effects of antimuscarinic
urinary incontinence only during the therapy with TL while
drugs since the detrusor contraction is reflex in such pa-
3 patients were incontinent with both the drugs but the uri-
tients and it is not influenced by psychological inhibition.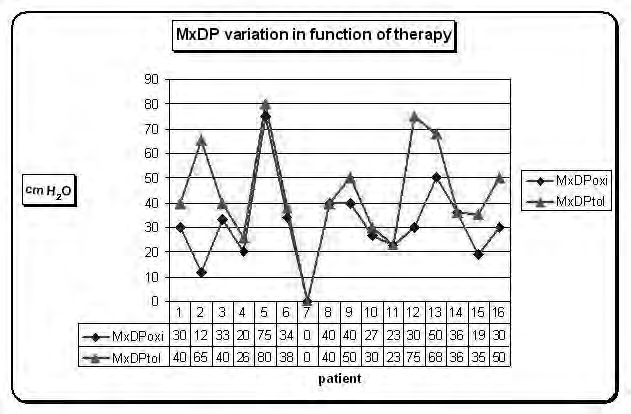 Elena Andretta, Bruno Bonadimani, Mauro Pastorello, Enrico Cossaro, Giorgio Artuso
Figure 2. – Maximum detrusor pressure (PMax) for any patient in consecutively treatment with oxybutynin and tolterodine.
Elena Andretta, Bruno Bonadimani, Mauro Pastorello, Enrico Cossaro, Giorgio Artuso
Figure 2. – Maximum detrusor pressure (PMax) for any patient in consecutively treatment with oxybutynin and tolterodine.