Relationship Between Platelet-Derived Growth Factor Expression in Leiomyomas and Uterine Volume Changes After Gonadotropin-ReleasingHormone Agonist Treatment
ANDREA DI LIETO, MD, GAETANO DE ROSA, MD,MARIANNA DE FALCO, MD, FRANCESCA IANNOTTI, MD,STEFANIA STAIBANO, MD, FABRIZIO POLLIO, MD,MARIANGELA SCARAMELLINO, MD,AND GAETANO SALVATORE, MD
The unopposed estrogen effect is the main cause of leiomyoma obtained fibroid samples. Uterine volume decreased significantly growth and is at the basis of the clinical use of gonadotropin-releasing after treatment, whereas just a poor modification was found in the hormone (GnRH) agonists. Platelet-derived growth factor (PDGF) controls. The decrease in the uterine volume was found to be statis- has been indicated as the main growth factor involved, in vitro in the tically related to PDGFexpression. Thus PDGFlevels decreased in proliferation response of leiomyoma smooth muscle cells to estrogen treated patients as compared with controls. The decreased PDGF stimulation. The aim of this article is to evaluate the mitogenic action production in leiomyomas after GnRH analogue treatment and the of PDGFin vivo by studying the relationship between PDGFexpres- relationship between decreased PDGFexpression and greater shrink- sion in leiomyomas and post-GnRH analogue treatment changes in age in uterine volume suggest that PDGFmight have a mitogenic action uterine volume. Thirty-nine patients suffering from uterine leiomyo- on leiomyomas in vivo. HUM PATHOL 33:220-224. Copyright 2002, mas were treated with leuprorelin acetate depot 3.75 mg for three Elsevier Science (USA). All rights reserved. cycles; 31 untreated patients were enrolled as control group. Uterine Key words: platelet-derived growth factor, leiomyoma, gonado- volume was determined twice by ultrasonography in each patient, the tropin-releasing hormone analogue. first time at admission and the second time after treatment in the Abbreviations: GnRH, gonadotropin-releasing hormone; PDGF, study group and after 3 months in the control group. The change in platelet-derived growth factor; EGF, epidermal growth factor; IGF, the uterine volume was then evaluated. Patients underwent surgery, insulin-like growth factor; E2, 17--estradiol; MAP, mitogen-activated and PDGFimmunohistochemical detection was performed on the protein.
Uterine leiomyomas are benign smooth muscle
of sex hormones at their target organs; therefore, they
cell tumors of the myometrium arising during the fe-
decrease sex hormone synthesis and secretion in long-
male reproductive period.1 The growth of these neo-
term treatment,9 with a subsequent pharmacologic hy-
plasms was shown to be dependent on the action of
poestrogenic state. A significant reduction in cellular
estrogen2 and progesterone3,4 and in some cases
proliferation was found in leiomyomas after GnRH ag-
associated with recently investigated chromosomal
changes.5,6 The unopposed estrogen effects on the
Sex steroid hormones seem to mediate their ac-
growth of leiomyomas are at the basis of the clinical use
tions on leiomyomas also through the autocrine and
of gonadotropin-releasing hormone (GnRH) agonists
paracrine effects of growth factors produced locally by
to reduce fibroid volume and to control symptoms such
smooth muscle cells and fibroblasts, such as epidermal
as menorrhagia, anemia, dysmenorrhea, and pelvic
growth factors (EGF and EGF-R),11-14 insulin-like
pressure,1,7,8 especially before a surgical procedure for
growth factors I and II (IGF-I and IGF-II),14-17 and
uterine leiomyomas. GnRH agonists induce pituitary
desensitization, through the downregulation of GnRH
Literature data on the effects of PDGF on uterine
receptors and the reduction of luteinizing and follicu-
fibroid progression are rather scarce. PDGF is synthe-
lar-stimulating hormones,7 and also inhibit the actions
sized and secreted by many cell types, including acti-vated vascular endothelial cells and macrophages, fi-broblasts, and smooth muscle cells under appropriate
From the Department of Obstetrical-Gynaecological and Urolog-
conditions.19 The expression of the PDGF- receptor in
ical Science and Reproductive Medicine and the Department of
numerous benign and malignant mesenchymal lesions
Biomorphological and Functional Science, Pathology Section, Uni-
suggests that PDGF might be involved in promoting
versity Federico II, Naples, Italy. Accepted for publication November19, 2001.
Address correspondence and reprint requests to Andrea Di Li-
Human myometrial tissue and myometrial smooth
eto, MD, Via L. Giordano, 120, 80127 Napoli, Italy.
muscle cells in primary culture locally produce EGF
Copyright 2002, Elsevier Science (USA). All rights reserved.
Some authors have demonstrated that both leiomyo-
PDGF EXPRESSION IN GnRH-a TREATED LEIOMYOMAS (Di Lieto et al)
mas and normal myometrium synthesize PDGF and
times in 10 mM of citrate buffer). After endogenous peroxi-
have assumed that this growth factor can act in an
dase activity was blocked, sections were preincubated with
autocrine or paracrine fashion.21 The PDGF- receptor
nonimmune mouse serum (1:20; Dakopatts, Glostrup, Den-
was found to coexist with PDGF in human leiomyo-
mark) diluted in PBS/BSA (1%) for 25 min at room temper-ature to prevent nonspecific bindings of antibodies. After
mas,19 and so changes in the synthesis or in the turn-
three washings with Tris buffer saline, the anti-PDGF (clone
over of this growth factor apparently play a role in
P-GF.44C; Novocastra, New Castle Upon Tyne, England) pri-
mary antibody was added, at 1:100 dilution, for an overnight
In a recent work,22 we demonstrated for the first
incubation at 4°C. As a positive control, the immunoreactivity
time that estrogen in vitro plays a key role in mediating
in a sample of human palatine tonsil was evaluated. Negative
the mitogenic effects on leiomyoma cells, by triggering
controls were performed in each run by substituting the
rapid and transient activation of the mitogen-activated
primary antibody with nonimmune serum (Dako Antibody
protein (MAP)– kinase pathway. Interestingly, the early
Diluent; Dakopatts). All of the slides were washed twice in
downstream signal transduction events determined
Tris-HCl buffer after each step. Sequential 20-min incuba-
tions with biotinylated link antibody and peroxidase-labelled
streptavidin (L.U. Dako LSAB kit, HRP) were then per-
induced PDGF secretion. PDGF was identified as the
formed. The chromgen 3,3Ј-diaminobenzidine (DAB; Vector
main growth factor involved in the proliferation re-
Laboratories, Burlingame, CA) was developed by the addition
sponse of leiomyoma muscle cells to estrogen stimula-
of 0.3% hydrogen peroxide. Nuclear counterstaining by he-
tion, upregulated by E2 and downregulated by anties-
matoxylin was performed; then sections were mounted and
cover slipped with a xylene-based mounting media (Entellan;
Basing on these findings about PDGF’s in vitro
Merck, Darmstadt, Germany). Immunostained sections were
action on human leiomyoma cells, in the present study
analyzed using a double-headed Leitz light microscope (ϫ40)
we evaluated the relationship between immunohisto-
in the most evenly and heavily labeled areas of the lesions,
chemical detection of PDGF in leiomyomas and post-
selected by inspection at low-power magnification with the aid
GnRH analogue treatment changes in uterine volume.
of a random table. A final 1000 cells were evaluated for eachcase and for each antibody. The average fraction of positivecells was determined and ranked on a semiquantitative scalebased on the percentage of cells with a definite nuclear
MATERIALS AND METHODS
staining, as follows: grade 0 (Ͻ 5%), grade 1 (5% to 25%),grade 2 (26% to 50%), and grade 3 (51% to 75%). All of the
Thirty-nine premenopausal women (mean age, 36.1 Ϯ
sections were examined without knowledge of the clinical and
3.2 [SD]; parity, 2.2 Ϯ 1.8) suffering from uterine leiomyomas
and referring to our Department of Obstetrical-Gynaecologi-
Patients were classified on the basis of the immunohisto-
cal and Urological Science and Reproductive Medicine gave
chemical grade for PDGF expression. The change in uterine
their informed consent to take part in the study. Patients were
volume (increase or shrinkage), defined as the ratio of the
treated with leuprorelin acetate depot 3.75 mg by monthly
second scanned volume minus the first scanned volume to
subcutaneous injection for three cycles, starting within the
the first scanned volume, was calculated for each immunohis-
first 7 days of the menstrual cycle, and then underwent uter-
tochemical grade. To assess the significance of the relation-
ine surgery. Thirty-one premenopausal women (mean age,
ship between the posttreatment modifications in the uterine
37.3 Ϯ 3.7; parity, 1.9 Ϯ 1.3) were enrolled as control group;
volume and the immunohistochemical grade for PDGF ex-
they received no GnRH agonist therapy and underwent sur-
pression, the change in uterine volume for each grade was
gery directly during the follicular phase of the menstrual
compared with that of the other grades.
cycle. No patient in the study or control group took hormonal
Data were analyzed by Fisher’s exact test (␣ ϭ 0.05) and
therapy, delivered, or underwent uterine surgery within 12
the Student t test (monodirectional hypothesis, ␣ ϭ 0.05).
months of the study or had malignant neoplasms.
Patients were submitted to bimanual examination, rou-
tine hematologic examinations, and ultrasonography. All of
the patients were scanned twice by transabdominal ultra-sonography, the first time at admission in both groups, and
All of the patients completed the therapy, thus
the second time after treatment in the study group and after
meeting the criteria to participate in the study. There
about 3 months in the control group. The uterine volume wascalculated using the formula of an ellipsoid.
All of the patients underwent surgery. In the study group,
21 patients underwent laparomiomectomy, 10 underwent
laparohisterectomy, and 8 underwent histeroscopic miomec-tomy. In the control group, 22 patients underwent laparo-
histerectomy and 9 underwent laparomiomectomy.
The surgical specimens were formalin fixed and paraffin
embedded, and then 4-m-thick serial sections were cut from
each block. One section was stained by hematoxylin and eosin
to confirm the histopathologic diagnosis. Immunocytochem-
istry was then performed on the remaining sections mounted
on poly-L-lysine– coated glass slides. To improve the stainingpattern, these sections were treated with the high-tempera-
NOTE. Data presented as mean (ϮSD).
ture antigen unmasking technique for paraffin sections (pre-
*Ratio of the second scanned volume minus the first scanned
incubation in a microwave oven at 650 watts for 5 min, three
volume to the first scanned volume. FIGURE 1.
Immunohistochemical grades for PDGF expression
in myomas of treated (o) and untreated (■) patients. FIGURE 3.
Immunohistochemical staining for PDGF in a GnRH
agonist–treated leiomyoma (grade 0). (Original magnification
was no significant difference between the groups withregard to age, parity, and uterine size. The uterinevolume decreased after Gn-RH analogue treatment. Inthe study group it was 571.3 Ϯ 266.7 cm3 (mean Ϯ SD)
with a mere appearance of increased cellular density,
at the first ultrasonographic scanning and 413.4 Ϯ 217
but in fact without nuclear atypia or mitotic activity.
cm3 after Gn-RH analogue administration, with a
In terms of the immunohistochemical detection of
shrinkage of 0.27 Ϯ 0.17. The difference between the
PDGF within the cytoplasm of smooth muscle cells and
first and second evaluations was found to be statistically
fibroblasts, in the study group 11 patients (28.2%) were
(Student t test, ␣ ϭ 0.05) significant. In the control
classified as grade 0, 16(41.1%) as grade 1, 8 (20.5%)
group, uterine volume was 540.4 Ϯ 250.8 cm3 at the
as grade 2, and 4 (10.2%) as grade 3. In the control
first evaluation and 601.1 Ϯ 241.3 cm3 at the second
group, 2 patients (6.5%) were classified as grade 0, 3
evaluation, with a statistically (Student t test) nonsignif-
icant increase of 0.1 Ϯ 0.2 (Table 1). In every patient,
(32.2%) as grade 3 (Figs 1, 2, and 3). The difference in
the uterine volume was different in the first and the
mean immunohistochemical grade between the study
group and the control group was found to be statisti-
The histologic features of the leiomyomas exam-
cally (Student t test) significant.
ined were those of typical leiomyomas, including inter-
The mean changes in uterine volume after GnRH
lacing bundles of smooth muscle cells and a variablecontent of fibroblasts and blood vessels. The histologic
analogue treatment were 0.36 Ϯ 0.19 (mean Ϯ SD) in
appearance of treated leiomyomas were similar in the
grade 0, 0.32 Ϯ 0.18 in grade 1, 0.14 Ϯ 0.03 in grade 2,
treated cases and the untreated cases. Only in nine
and 0.09 Ϯ 0.006in grade 3 (Table 2).
cases (23%) was considerable nuclear crowding found,
Patients with a lower PDGF expression (i.e., a low
immunohistochemical grade) showed a higher volumedecrease after GnRH analogue administration. The re-lationship between the grades with regard to the per-centage of shrinkage in uterine volume after treatmentwas found to be statistically (Student t test) significant,except for the comparison between grade 0 and grade1 (Table 3).
change*(mean Ϯ SD) 0.36 Ϯ 0.19 0.32 Ϯ 0.18 0.14 Ϯ 0.03 0.09 Ϯ 0.006
FIGURE 2.
Immunohistochemical staining for PDGF in an un-
*Ratio of the second scanned volume minus the first scanned
treated leiomyoma. (Original magnification ϫ250.)
volume to the first scanned volume.
PDGF EXPRESSION IN GnRH-a TREATED LEIOMYOMAS (Di Lieto et al)
GnRH analogue–treated uterine leiomyomas27 re-
ported cellular atrophy due to a decrease in myofila-
ments, mithocondrial swelling, and emergence of thelysosomal body. Finally, the decrease in cell prolifera-
tion, indicated by reduced expression of proliferating
cell nuclear antigen and of nuclear antigen Ki67, was
demonstrated in uterine leiomyomas after GnRH ana-
The decrease in uterine volume observed in our
study seems to be significantly related to the PDGF
Abbreviations: S, significant; NS, nonsignificant. NOTE. Student t test, monodirectional hypothesis, ␣ ϭ 0.05.
expression in leiomyoma cells. The comparison be-tween the immunohistochemical grades with regard tothe uterine volume changes was found to be statistically
DISCUSSION
significant, except for the relationship between grade 0and grade 1.
The presence of RNA transcripts for PDGF21,23 and
At the beginning of the study, the two groups
for PDGF receptors20 has been demonstrated in normal
statistically belonged to the same population. The
myometrium. In vitro studies20 have shown that myo-
mean immunohistochemical grade was significantly
metrial smooth muscle cells in culture are responsive to
higher in controls than in treated patients. In the con-
the mitogenic action of PDGF, independent of the
trol group, a high PDGF expression prevailed (with
phases of the menstrual cycle. The detection of PDGF
most patients classified as grade 2 or 3), whereas the
in human leiomyomas19,21 and the coexpression of
treated patients were mostly classified as grade 0 or 1,
PDGF and PDGF- receptor19 suggested the involve-
thus showing low PDGF expression. This brings us to
ment of this growth factor with mitogenic effects in the
hypothesize that GnRH analogue treatment actually
caused reduced PDGF synthesis in leiomyoma cells.
In a recent study22 we reported the results of in
PDGF expression was significantly reduced in those
vitro experiments demonstrating that E2 acts by induc-
treated patients who exhibited a greater uterine vol-
ing the production of growth factors and determines
ume decrease. Then, the “nonresponders” mechanism
transduction events related to the estrogen-induced
might be related to a low tissue and receptor response
PDGF secretion. Moreover, we demonstrated that
to GnRH analogue; this is made more evident by the
PDGF had a main role in the proliferative activity of
absence of reduced PDGF levels after treatment.
leiomyoma smooth muscle cells. Antiestrogen cell treat-
The assumption of GnRH analogue–induced de-
ment is correlated with the disappearance of the mito-
crease in PDGF synthesis by leiomyoma cells and the
genic factor, PDGF, in leiomyoma smooth muscle cell–
demonstration that this lower expression is significantly
conditioned media, whereas the E2 mitogenic action is
related to the post-GnRH analogue treatment shrink-
almost completely neutralized by anti-human PDGF
age in the uterine volume suggest that PDGF might
antibodies, suggesting the direct involvement of this
have a mitogenic in vivo action on leiomyomas. In
growth factor in leiomyoma proliferation.
addition, we confirm the presence of PDGF within the
Because the interaction between estrogen and
cytoplasm of leiomyomatous smooth muscle cells and
PDGF in leiomyoma progression has been demon-
of fibroblasts, but not in the extracellular matrix.21 The
strated in vitro, and considering the pharmacologic
absence of deposition in the extracellular matrix might
effects of GnRH analogues, an in vivo mitogenic action
indicate that PDGF has a local autocrine or paracrine
of PDGF on leiomyomas is suggested by a significant
action. Even if further studies on a greater number of
relationship between the shrinkage in uterine volume
patients are necessary, our results can integrate the
and the decrease in PDGF synthesis, as a result of the
findings about the PDGF role on leiomyoma progres-
GnRH analogue–induced hypoestrogenic state.
sion that have been well demonstrated in vitro.
All of the data collected in the present study con-
firm that GnRH analogue treatment causes a significantshrinkage in uterine volume.24,25 The histologic fea-
REFERENCES
tures of treated leiomyomas do not appear to be relatedto the variable response to the analogue therapy. The
1. Lethaby A, Vollenhoven B, Sowter M: Pre-operative GnRH
most important difference that we found between
analogue therapy before hysterectomy or myomectomy for uterine
treated and untreated cases was the marked nuclear
fibroids. Cochrane Database Syst Rev 2:CD000547, 2000
crowding observed in some samples from treated
2. Brandon DD, Erckson TE, Keenan EJ, et al: Estrogen receptor
gene expression in human uterine leiomyomas. Biol Reprod 80:1876-
leiomyomas. These findings might indicate a decrease
in either the cytoplasmic volume or the interstitial
3. Brandon DD, Bethers CL, Strawn EY, et al: Progesterone
ground substance.26 Furthermore, the shrinkage in
receptor messenger ribonucleic acid and protein are overexpressed
leiomyoma volume resulting from GnRH analogue
in human uterine leiomyomas. Am J Obstet Gynecol 169:78-85, 1993
therapy might be related to ultrastructural modifica-
4. Rein MS, Barbieri RL, Friedman AJ: Progesterone: A critical
role in the pathogenesis of uterine myomas. Am J Obstet Gynecol
tions, not assessed in the present study. As a matter of
fact, a recent study on the ultrastructural features of
5. Henning Y, Caselitz J, Stern C, et al: Karyotype evolution in a
case of uterine angioleiomyoma. Cancer Genet Cytogenet 108:79-80,
factor I promotes leiomyoma cell growth in vitro. Am J Obstet Gy-
6. Mantovani MS, Neto JB, Philbert PM, et al: Multiple uterine
17. Giudice LC, Irwin JC, Duspin BA, et al: Insulin-like growth
leiomyomas: Cytogenetic analysis. Gynecol Oncol 72:71-75, 1999
factor (IGF), IGF-binding protein (IGFBP) and IGF receptor gene
7. Filicori M, Hall DA, Loughlin JS, et al: A conservative ap-
expression and IGFBP synthesis in human uterine leiomyomata.
proach to the management of uterine leiomyoma: Pituitary desensi-
tization by a luteinizing hormone-releasing hormone analogue. Am J
18. Fayed YM, Tsibris JCM, Langenberg PW, et al: Human uter-
ine leiomyoma cells: Binding and growth responses to epidermal
8. Crow J, Gardner RL, McSweeney G, et al: Morphological
growth factor, platelet-derived growth factor and insulin. Lab Invest
changes in uterine leiomyomas treated by GnRH agonist goserelin.
19. Palman C, Bowen-Pope DF, Brooks JJ: Platelet-derived
9. Pa`lyi I, Vincze B, Lovas S, et al: Gonadotropin-releasing hor-
growth factor receptor (-subunit) immunoreactivity in soft tissue
mone analogue conjugates with strong selective antitumor activity.
Proc Natl Acad Sci USA 96:2361-2366, 1999
20. Rossi MJ, Chegini N, Masterson BJ: Presence of epidermal
10. Vu K, Greenspan DL, Wu TC, et al: Cellular proliferation,
growth factor, platelet-derived growth factor, and their receptors in
estrogen receptor, progesterone receptor, and bcl-2 expression in
human myometrial tissue and smooth muscle cells in vitro. Endocri-
GnRH agonist-treated uterine leiomyomas. H
21. Mangrulkar RS, Ono M, Ishikawa M, et al: Isolation and
characterization of heparin-binding growth factors in human
11. Di Lieto A, De Rosa G, Albano G, et al: Hormonal therapies
leiomyomas and normal myometrium. Biol Reprod 53:636-646, 1995
and EGF-R expression in the human mammary gland. Breast Dis
22. Barbarisi A, Petillo O, Di Lieto A, et al: 17- estradiol elicits
an autocrine leiomyoma cell proliferation: Evidence for a stimulation
12. Yeh J, Rein M, Nowak R: Presence of messenger ribonucleic
of protein kinase-dependent pathway. J Cell Physiol 186:414-424,
acid for epidermal growth factor (EGF) and EGF receptor demon-
strable in monolayer cell cultures of myometria and leiomyomata.
23. Bohem KD, Daimon M, Gorodeski IG, et al: Expression of
the insulin-like and platelet-derived growth factor genes in human
13. Harrison-Woolrych ML, Charnock-Jones DS, Smith SK:
uterine tissues. Mol Reprod Devel 27:93-101, 1995
Quantification of messenger ribonucleic acid for epidermal growth
24. Lumsden MA, West CP, Baerd DT: Goserelin therapy before
factor in human myometrium and leiomyomata using reverse-tran-
surgery for uterine fibroids. Lancet 1:36-37, 1997
scription polymerase chain reaction. J Clin Endocrinol Metab 78:
25. Friedman AJ, Lobel SM, Rein MS: Efficacy and safety con-
siderations in women with uterine leiomyomas treated with gonado-
14. Dixon D, Haseman JK: Immunohistochemical localization of
tropin-releasing hormone agonists: The estrogen threshold hypoth-
growth factors and their receptors in uterine leiomyomas and
esis. Am J Obstet Gynecol 163:1114-1119, 1990
matched myometrium. Environ Health Perspect 108(S5):795-802,
26. Colgan TJ, Pendergast S, LeBlanc M: The histopathology of
uterine leiomyomas following treatment with gonadotropin-releasing
15. Rein MS, Friedman AJ, Pandian MR, et al: The secretion of
hormone analogues. HUM PATHOL 24:1073-1077, 1993
insulin-like growth factors I and II explant cultures of fibroids and
27. Ito F, Kawamura N, Ichimura T, et al: Ultrastructural com-
myometrium from women treated with gonadotropin-releasing hor-
parison of uterine leiomyoma cells from the same myoma nodule
mone agonist. Obstet Gynecol 76:388-394, 1990
before and after gonadotropin-releasing hormone agonist treatment.
16. Strawn EY, Novy MJ, Burry KA, et al: Insulin-like growth
Linee e fermate abilitate al servizio disabili sulla rete urbana di Trento Piazza Dante "Stazione FS" Gandhi "Parco Anna Frank" S.Francesco Porta Nuova Gramsci "Materna la Clarina" dei Mille "Villa Igea" Gocciadoro "Poliambulatori" Gorizia Adamello "Gocciadoro Arcate" Bolghera "S.Antonio" Gerola "Osp. S.
PSP and CBD for General Practitioners and Community Nurses Working for a World Free of PSP PSP and CBD for General Practitioners and Community Nurses This booklet is part of a series of new publications for health and social care professionals, to help them support people who have Progressive Supranuclear Palsy (PSP) and Cortico Basal Degeneration (CBD). The PSP Association
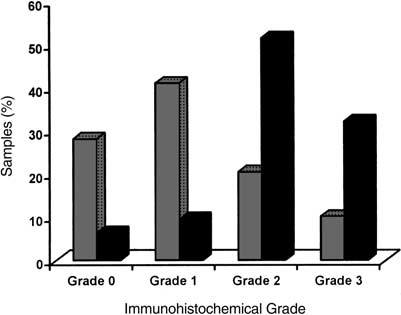
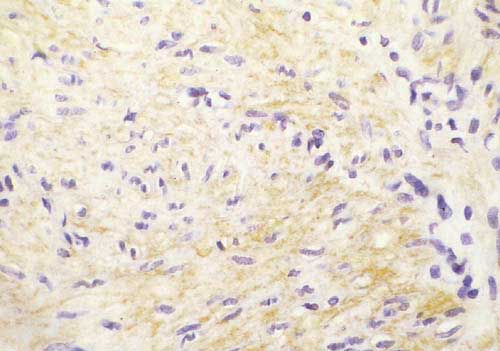
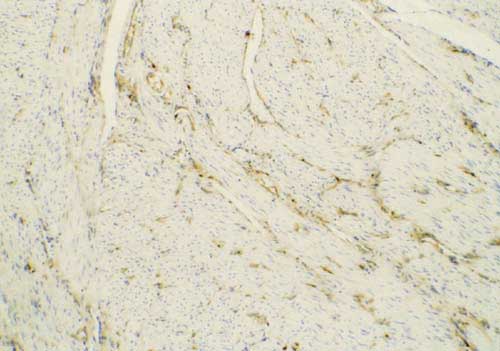 FIGURE 1.
FIGURE 1.