The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Pathophysiology
The most frequent form of venous gas embolism
is the insidious venous aeroembolism, in which a se-ries of gas bubbles resembling a string of pearls en-
GAS EMBOLISM
ters the venous system. Rapid entry or large volumesof gas put a strain on the right ventricle because of
CLAUS M. MUTH, M.D., AND ERIK S. SHANK, M.D.
the migration of the emboli to the pulmonary circu-lation. The pulmonary arterial pressure increases, andthe increased resistance to right ventricular outflowcauses diminished pulmonary venous return. Because
AS embolism, the entry of gas into vascular
of the diminished pulmonary venous return, there is
structures, is a largely iatrogenic clinical prob-
decreased left ventricular preload, resulting in dimin-
lem that can result in serious morbidity and
ished cardiac output and, ultimately, systemic cardio-
even death.1 Since gas embolism can result from pro-
vascular collapse.9 Tachyarrhythmias often develop,
cedures performed in almost all clinical specialties
but bradycardias are possible as well. When large quan-
(Table 1), it is important for all clinicians to be aware
tities of gas (over 50 ml) are injected abruptly, acute
of this problem. In most cases, gas embolism is air
cor pulmonale, asystole, or both are likely to occur.2
embolism, although the medical use of other gases,
The alteration in the resistance of the lung vessels and
such as carbon dioxide, nitrous oxide, and nitrogen,
the mismatch between ventilation and perfusion cause
can also result in the condition. There are two broad
intrapulmonary right-to-left shunting and increased
categories of gas embolism, venous and arterial, which
alveolar dead space, leading to arterial hypoxia and
are distinguished by the mechanism of gas entry and
the site where the emboli ultimately lodge. Diagnosis VENOUS GAS EMBOLISM
To diagnose venous gas embolism, the physician
Venous gas embolism occurs when gas enters the
should assess the clinical findings. The so-called mill-
systemic venous system.2 The gas is transported to
wheel murmur, a splashing auscultatory sound due
the lungs through the pulmonary arteries, causing
to the presence of gas in the cardiac chambers and
interference with gas exchange, cardiac arrhythmias,
great vessels, is often present and can be auscultated
pulmonary hypertension, right ventricular strain, and
by a precordial or esophageal stethoscope. A decrease
eventually cardiac failure. Physical preconditions for
in the end-tidal carbon dioxide levels, as determined
the entry of gas into the venous system are the in-
by capnometry, suggests a change in the relation be-
cising of noncollapsed veins and the presence of sub-
tween ventilation and perfusion due to the obstruc-
atmospheric pressure in these vessels. Noncollapsing
tion of the pulmonary arteries.10 Doppler ultrasonog-
veins include the epiploic veins, the emissary veins,
raphy is a sensitive and practical means of detecting
and the dural venous sinuses. Air may enter these
intracardiac air, and it is often used during neurosur-
veins during neurosurgical operations, especially those
gical procedures,3,11 procedures with the patient in
performed with the patient in the sitting position.3
the sitting position, and other procedures that entail
The veins of the throat, and in some cases the veins
a high risk of gas embolism. An even more sensitive
in the coagulated operative field,4 may also be entry-
and definitive method for detecting intracardiac gas
ways for air. Air may also enter veins through central
is transesophageal echocardiography, although it re-
venous and hemodialysis catheters5,6 and may enter
quires training in performance and interpretation
the veins of the myometrium during pregnancy and
Treatment
When venous gas embolism is suspected, further
entry of gas must be prevented. In certain cases,
From the Druckkammerzentrum Homburg, University Hospital Hom-
therapy with catecholamines is required, and, if nec-
burg, University of the Saarland, Homburg/Saar, Germany (C.M.M.); and
essary, aggressive cardiopulmonary resuscitation is per-
the Department of Anesthesiology and Critical Care, Massachusetts Gen-eral Hospital and the Department of Anesthesiology, Harvard Medical
formed. Adequate oxygenation is often possible only
School — both in Boston (E.S.S.). Address reprint requests to Dr. Muth at
with an increase in the oxygen concentration of the
the Druckkammerzentrum Homburg, Universitätskliniker des Saarlandes,
inspired gas (up to 100 percent oxygen). Supplemen-
66424 Homburg/Saar, Germany, or at [email protected].
2000, Massachusetts Medical Society.
tal oxygen also reduces the size of the gas embolus
P R I M A RY C A R E TABLE 1. MEDICAL SPECIALTIES WITH DOCUMENTED CASES OF GAS EMBOLISM. SPECIALTY MECHANISM OF GAS EMBOLISM
Inadvertent entry of air through peripheral intravenous circuit
Intraoperative use of hydrogen peroxide, causing formation of arterial and venous oxygen emboli
Entry of air through disconnected intravascular catheter, inadvertent infusion of air through intravascu-
Entry of air into extracorporeal-bypass pump circuit, incomplete removal of air from heart after cardio-
plegic arrest, carbon dioxide–assisted harvesting of peripheral veins
Entry of air through intravascular catheter during angiographic study or procedure
Entry of air through disconnected intravascular catheter, pulmonary barotrauma, rupture of intraaortic
balloon, entry of air into extracorporeal-membrane-oxygenator circuit
Pulmonary barotrauma, paradoxical embolism after decompression injury, entry of gas through discon-
Entry of gas into veins or arteries during insufflation of body cavities
Entry of gas into veins during upper or lower endoscopy or endoscopic retrograde pancreatography
Pulmonary barotrauma in treatment of premature infants
Inadvertent entry of air through hemodialysis catheter and circuit on hemodialysis machine
Entry of air through incised veins and calvarial bone, especially during craniotomy with the patient in
Cesarean section, gas insufflation into veins during endoscopic surgery, intravaginal and intrauterine gas
Nd:YAG laser surgery on the larynx, trachea, or bronchi*
Gas insufflation into veins during arthroscopy, total hip arthroplasty, or spine surgery with the patient
Injection of air or gas as a contrast agent, inadvertent injection of air during angiography
Entry of air into pulmonary vasculature during lung biopsy or video-assisted thoracoscopy, chest trauma
(penetrating or blunt), lung transplantation
Entry of air during transurethral prostatectomy or radical prostatectomy
Entry of air during carotid endarterectomy
*Nd:YAG denotes neodymium:yttrium–aluminum–garnet.
by increasing the gradient for the egress of nitrogen
toms of end-artery obstruction. There are a number
from the bubble.13 Rapid resuscitation with volume
of mechanisms by which this can occur. One is the
expansion is recommended to elevate venous pres-
passage of gas across a patent foramen ovale into the
sure, thus preventing the continued entry of gas into
systemic circulation. A patent foramen ovale, which
is detectable in about 30 percent of the general pop-
Some authors recommend attempting to evacuate
ulation, makes possible right-to-left shunting of gas
air from the right ventricle with the use of a central
bubbles.16 If there is a patent foramen ovale and if
venous catheter (a multiorifice catheter may be more
the pressure in the right atrium exceeds the pressure
effective than one with a single lumen) or a pulmo-
in the left atrium, right-to-left flow through the fo-
nary arterial catheter.2,14,15 It may be possible to as-
ramen ovale may occur.17 Elevated pulmonary arte-
pirate about 50 percent of the entrained air from an
rial pressure due to venous gas embolism may result
appropriately placed right atrial catheter,2,14 but de-
in elevated right atrial pressure, making it possible
pending on the placement of the catheter and the
for a bubble to be transported through a patent fo-
position of the patient, a smaller effect is more like-
ramen. Furthermore, the decrease in left atrial pres-
ly.2,15 Hyperbaric oxygen therapy is not a first-line
sure caused by controlled ventilation and the use of
treatment but may be a useful adjunct in severe cas-
positive end-expiratory pressure may create a pressure
es. It should certainly be considered if there is evi-
gradient across the patent foramen ovale, favoring the
dence of neurologic changes. In this case, it should
passage of gas into the systemic circulation.2,3
be assumed that a paradoxical embolism is present.
In other situations, venous gas may enter the ar-
terial circulation by overwhelming the mechanisms
Paradoxical Embolism
that normally prevent arterial gas embolism. Studies
A paradoxical embolism occurs when air or gas
in animals suggest that either a large bolus of gas (20
that has entered the venous circulation manages to
ml or more) or small continuous amounts (11 ml
enter the systemic arterial circulation and causes symp-
per minute) introduced into the venous system may
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Pathophysiology
The entry of gas into the aorta causes the distri-
bution of gas bubbles into nearly all organs. Small em-boli in the vessels of the skeletal muscles or visceraare well tolerated, but embolization to the cerebral orcoronary circulation may result in severe morbidityor death.
Embolization into the coronary arteries induces
electrocardiographic changes typical of ischemia andinfarction; dysrhythmias, myocardial suppression, car-diac failure, and cardiac arrest are all possible, depend-ing on the amount of gas embolized.25 Circulatoryresponses may also be seen with embolization to thecerebral vessels.26
Cerebral arterial gas embolization typically involves
the migration of gas to small arteries (average diam-eter, 30 to 60 µm).25 The emboli cause pathologic
Figure 1. Transesophageal Echocardiogram from a Patient Eval- uated for the Presence of a Patent Foramen Ovale.
changes by two mechanisms: a reduction in perfusion
Saline was agitated and injected rapidly into a central venous
distal to the obstruction and an inflammatory response
catheter. The bubbles appear as echodense areas in the right
atrium (double arrows). If this patient had a patent foramenovale, bubbles would be seen crossing the interatrial septum
Symptoms
(thin arrow) and entering the left atrium (arrowhead). (Echocar-
The symptoms of cerebral arterial gas embolism
diogram provided courtesy of S. Streckenbach.)
develop suddenly. The clinical presentation, however,is determined by the absolute quantity of gas and theareas of the brain that are affected. Thus, there may
generate intraarterial bubbles.18-20 There have been
be minor motor weakness and headache or moderate
reports of fatal cerebral arterial gas embolism caused
confusion; conversely, complete disorientation, hem-
by a large venous gas embolus, although no intracar-
iparesis, convulsions, loss of consciousness, and coma
diac defects or shunt mechanisms could be demon-
may occur.27 Asymmetry of the pupils, hemianopia,
strated.21 Various anesthetic agents diminish the ability
and impairment of the respiratory and circulatory cen-
of the pulmonary circulation to filter out gas embo-
ters (manifested as bradypnea, Cheyne–Stokes breath-
li.22 Studies in animals have shown that volatile anes-
ing, cardiac arrhythmias, and circulatory failure)25,26
thetics, specifically, may raise the threshold for a spill-
are other well-known complications. In patients who
over of venous bubbles into systemic arteries. This
have undergone surgical procedures that carry a risk of
finding may have relevance to surgical procedures that
gas embolism, a delayed recovery from general anes-
carry a substantial risk of venous gas embolism.
thesia or a transitional stage of impaired consciousness
The treatment of paradoxical embolism is identi-
may be a clue to the occurrence of cerebral arterial
cal to that of primary arterial gas embolism (discussed
gas embolism. The diagnosis is not easy to establish
below). Every venous gas embolism has the poten-
in such patients, because complications of anesthesia,
tial to evolve into an arterial gas embolism.
such as the central anticholinergic syndrome or thepresence of residual anesthetic or muscle relaxant, can
ARTERIAL GAS EMBOLISM
mimic mild cerebral arterial gas embolism.
Arterial gas embolism is caused by the entry of gas
into the pulmonary veins or directly into the arteries
Diagnosis
of the systemic circulation. Gas may enter the arteries
The most important diagnostic criterion is the pa-
as a result of overexpansion of the lung by decompres-
tient’s history, because the clinical suspicion of em-
sion barotrauma or as a result of paradoxical embo-
bolism is based on the initial neurologic symptoms
lism. Any cardiac surgical operation that uses extracor-
and the direct temporal relation between these symp-
poreal bypass may also cause arterial gas embolism.23
toms and the performance of an invasive procedure.
Even if only small amounts of gas enter the arterial
The procedures that carry the greatest risk of venous
system, the flow of gas bubbles into functional end
or arterial gas embolism are craniotomy performed
arteries occludes these vessels. Although obstruction
with the patient in the sitting position, cesarean sec-
is possible in any artery, obstruction of either the
tion, hip replacement, and cardiac surgery with car-
coronary arteries or the nutritive arteries of the brain
diopulmonary bypass. All these procedures have in
(cerebral arterial gas embolism) is especially serious
common an incised vascular bed and a hydrostatic
and may be fatal because of the vulnerability of the
gradient favoring the intravascular entry of gas.
heart and brain to short periods of hypoxia.24
Cerebral arterial gas embolism can sometimes be
P R I M A RY C A R E Figure 2. Bubble Obstructing End-Arterial Flow in a Cerebral Vessel with a Diameter of 30 to 60 µm, Causing Distal Ischemia.
The obstruction causes the metabolic processes of neurons to fail. Sodium and water enter the vessel, and cytotoxic edema devel-ops. The surface of the bubble generates a foreign-body response through cellular and humoral immune mechanisms. The bubblealso mechanically irritates the arterial endothelium. Both processes result in vasogenic edema and greater impairment of perfusion. The neuronal injury extends beyond the area of obstruction.
distinguished from a cerebral infarct or intracerebral
diovascular system. Endotracheal intubation should
bleeding on a computed tomographic (CT) scan.28
be performed in a somnolent or comatose patient in
However, pathologic changes are sometimes very sub-
order to maintain adequate oxygenation and ventila-
tle and not well visualized on CT, and the diagnosis
tion. Oxygen should also be administered, at as high
of cerebral arterial gas embolism must be considered
a concentration as possible.30 Administration of oxy-
early. Magnetic resonance imaging of the cerebrum
gen is important not only to treat hypoxia and hypox-
can sometimes show an increased volume of water
emia but also to eliminate the gas in the bubbles by
concentrated in the injured tissue. But this method
establishing a diffusion gradient that favors the egress
is also not reliable and may fail to detect an embo-
It is currently recommended that patients with ar-
Gas bubbles in the vessels of the retina can occa-
terial gas embolism be placed in the flat supine po-
sionally be identified, but their absence does not rule
sition.31 The buoyancy of gas bubbles is not sufficient
out gas embolism.24 Another finding that is nonspe-
to counteract blood flow propelling such bubbles to-
cific but that has been described in a number of cases
ward the head, even when the patient is placed in a
is hemoconcentration with an increase in the hema-
head-down position. In addition, the head-down po-
tocrit, possibly as a direct consequence of the extravas-
sition may aggravate the cerebral edema that develops
cular shift of fluid into the injured tissues.29
Treatment Treatment of Generalized Seizures
The primary goal of treatment is the protection
Cerebral gas embolism often causes generalized
and maintenance of vital functions. If necessary, car-
seizures,27 which may not respond to benzodiaze-
diopulmonary resuscitation should be performed,
pines. In these cases, it is recommended that the sei-
since not only venous but also primary arterial gas
zures be suppressed with barbiturates.27,33 Although
embolism may lead to serious impairment of the car-
there is no proof that barbiturates provide cerebral
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
protection after cerebral ischemia, the use of barbi-
turates for ischemic brain lesions has certain advan-
tages. They reduce cerebral oxygen consumption, in-
tracranial pressure, the production of free radicals, and
the release of endogenous catecholamines.34,35 High
doses of barbiturates depress respiration; ventilatory
support must therefore be available when a patient
Hyperbaric-Oxygen Therapy
With hyperbaric-oxygen therapy, the patient
breathes 100 percent oxygen at a pressure above that
of the atmosphere at sea level. This therapy decreasesthe size of the gas bubble both by raising the ambi-
Figure 3. Relation between the Size of the Bubble and Pressure.
ent pressure (Fig. 3) and by causing systemic hyperox-
The surface area and volume of the gas bubble are inverselyproportional to pressure at a constant temperature (Boyle’s law).
ia. An arterial partial pressure of oxygen greater than
Thus, as the patient is exposed to increasing ambient pressure,
2000 mm Hg is frequently achieved. The hyperoxia
produces enormous diffusion gradients for oxygeninto the bubble and for nitrogen out of the bub-ble.31,32 The hyperoxia also allows much larger quan-tities of oxygen to be dissolved in the plasma and in-
may become the first choice for volume replacement,
creases the extent of oxygen diffusion in tissues.27
but their use is still controversial and therefore can-
The improvements in the oxygen-carrying capacity
of plasma and in the delivery of oxygen to tissues
The goal of infusion therapy is normovolemia.
offset the embolic insult to the microvasculature.
Placement of a central venous catheter is strongly
Other benefits of hyperbaric oxygen have been
recommended to assess central venous pressure, which
proposed. It may help prevent cerebral edema by re-
should be maintained at approximately 12 mm Hg.
ducing the permeability of blood vessels while sup-
As a further method of ensuring adequate volume
porting the integrity of the blood–brain barrier.36,37
status, the urinary output should be monitored with
Furthermore, experiments have suggested that hyper-
a Foley catheter and maintained above 1 to 2 ml per
baric oxygen diminishes the adherence of leukocytes
These benefits suggest that all patients with clini-
Anticoagulant Therapy
cal symptoms of arterial gas embolism should receive
There is evidence that heparin may be beneficial in
recompression treatment with hyperbaric oxygen. Al-
the treatment of gas embolism.42 Studies have shown
though immediate recompression produces the best
that the clinical course of arterial gas embolism is
response,23 delayed treatment in a hyperbaric cham-
less severe if the patient has been treated with hep-
ber may still be indicated to ameliorate the patient’s
arin before the embolic event occurs. An argument
condition.39 Hyperbaric oxygen is the first-line treat-
against heparin therapy is the risk it entails of hem-
ment of choice for arterial gas embolism.23,25,31,40 Thus,
orrhage into the infarcted tissue. At present, the use
as soon as cardiopulmonary stabilization has been
of heparin for the short-term treatment of cerebral
achieved, the patient should be transferred to a hy-
arterial gas embolism is not generally recommended. Corticosteroid Therapy Infusion Therapy
The use of corticosteroids in patients with arterial
There is some evidence that gas embolism may
gas embolism remains controversial. Some authors
cause hemoconcentration, which increases blood vis-
recommend treatment with corticosteroids to com-
cosity and impairs the already compromised micro-
bat the brain edema43 that results from gas emboliza-
circulation.29 Therefore, normovolemia should be
tion in the cerebral arteries. Cerebral gas embolism ini-
achieved to optimize the microcirculation. Hypovo-
tially induces the rapid development of cytotoxic brain
lemia is always tolerated less well than relative ane-
edema, with diminished extracellular space and en-
mia. It is therefore acceptable to decrease the hem-
larged intracellular areas. This form of edema does not
atocrit, within certain limits. In animals, moderate
usually respond to corticosteroids.44 Some authors re-
hemodilution to a hematocrit of 30 percent reduces
port that corticosteroids aggravate ischemic injury after
neurologic damage.41 Colloid solutions are preferable
occlusion of the vessels.45,46 Thus, since corticoster-
to crystalloid solutions for hemodilution, because the
oids appear to offer no benefit in patients with cyto-
latter may promote cerebral edema. Hypertonic so-
toxic edema and since these drugs may aggravate neu-
lutions (e.g., 7.5 percent sodium chloride solution)
ronal ischemic injury, we do not recommend them. P R I M A RY C A R E TABLE 2. TREATMENT OF GAS EMBOLISM. TYPE OF TREATMENT VENOUS GAS EMBOLISM ARTERIAL GAS EMBOLISM
Measures to increase venous pressure (e.g., Valsalva
Identification and shutting down of entryway
maneuver or intravenous administration of fluids)
Identification and shutting down of entryway for gas
Hyperbaric oxygen therapy as soon as patient’s
condition is stable enough for transfer to hyperbaric chamber
Aspiration with multiluminal central venous catheter
(with patient in left lateral decubitus position)
Lidocaine, antiepileptic agents, physical therapy
Lidocaine Therapy 2. Palmon SC, Moore LE, Lundberg J, Toung T. Venous air embolism: a review. J Clin Anesth 1997;9:251-7.
Although the results of clinical studies of lidocaine
3. Porter JM, Pidgeon C, Cunningham AJ. The sitting position in neuro-
for the treatment of arterial gas embolism are not yet
surgery: a critical appraisal. Br J Anaesth 1999;82:117-28. 4. Donlon JV Jr. Anesthesia and eye, ear, nose, and throat surgery. In: Mil-
available, studies in animals suggest that lidocaine may
ler RD, ed. Anesthesia. 3rd ed. Vol. 2. New York: Churchill Livingstone,
be beneficial.47-51 In animals given prophylactic doses
of lidocaine, the depressant effects of gas embolism on
5. Halliday P, Anderson DN, Davidson AI, Page JG. Management of cer- ebral air embolism secondary to a disconnected central venous catheter. Br
somatosensory evoked potentials and the elevations
in intracranial pressure caused by gas embolism were
6. Yu AS, Levy E. Paradoxical cerebral air embolism from a hemodialysis
both reduced. In a clinical trial, lidocaine provided
catheter. Am J Kidney Dis 1997;29:453-5. 7. Hill BF, Jones JS. Venous air embolism following orogenital sex during
cerebral protection during cardiac surgery.51 There-
pregnancy. Am J Emerg Med 1993;11:155-7.
fore, a strong argument can be made for administer-
8. Weissman A, Kol S, Peretz BA. Gas embolism in obstetrics and gyne- cology: a review. J Reprod Med 1996;41:103-11.
ing lidocaine in a bolus dose of 1.5 mg per kilogram
9. Durant TM, Long J, Oppenheimer MJ. Pulmonary (venous) air embo-
and maintaining a therapeutic concentration, with
continuous intravenous administration in patients with
10. Shapiro HM, Drummond JC. Neurosurgical anesthesia and intracra- nial hypertension. In: Miller RD, ed. Anesthesia. 3rd ed. Vol. 2. New York:
severe arterial gas embolism. However, an overdose
Churchill Livingstone, 1990:1737-89.
of lidocaine may cause central nervous system depres-
11. Gildenberg PL, O’Brien RP, Britt WJ, Frost EA. The efficacy of Dop-
sion, cerebral convulsions, and bradyarrhythmias.
pler monitoring for the detection of venous air embolism. J Neurosurg 1981;54:75-8. 12. Mammoto T, Hayashi Y, Ohnishi Y, Kuro M. Incidence of venous and CONCLUSIONS
paradoxical air embolism in neurosurgical patients in the sitting position: detection by transesophageal echocardiography. Acta Anaesthesiol Scand
The entry of gas into the venous or arterial system
is a risk in virtually all areas of clinical care. Venous
13. Van Liew HD, Conkin J, Burkard ME. The oxygen window and de-
emboli may lead to cardiovascular collapse or to par-
compression bubbles: estimates and significance. Aviat Space Environ Med 1993;64:859-65.
adoxical arterial emboli. Arterial emboli may occlude
14. De Angelis J. A simple and rapid method for evacuation of embolized
end arteries throughout the body and may cause se-
rious morbidity or death if they occlude cardiac or
15. Albin MS. Air embolism. In: Albin MS, ed. Textbook of neuroanes- thesia with neurosurgical and neuroscience perspectives. New York:
Regardless of the mechanism responsible for the
16. Lynch JJ, Schuchard GH, Gross CM, Wann LS. Prevalence of right- to-left atrial shunting in a healthy population: detection by Valsalva maneu-
embolism, rapid and aggressive treatment is essential
ver contrast echocardiography. Am J Cardiol 1984;53:1478-80.
to preserve life and function (Table 2). For venous gas
17. Gronert GA, Messick JM Jr, Cucchiara RF, Michenfelder JD. Paradox-
embolism, the mainstays of treatment are the pre-
ical air embolism from a patent foramen ovale. Anesthesiology 1979;50:548-9.
vention of further entry of gas, volume expansion,
18. Butler BD, Hills BA. The lung as a filter for microbubbles. J Appl
the administration of 100 percent oxygen, often with
ventilatory support; positive inotropic support; and
19. Vik A, Brubakk AO, Hennessy TR , Jenssen BM, Ekker M, Slørdahl SA. Venous air embolism in swine: transport of gas bubbles through the
cardiopulmonary resuscitation, if necessary. For ar-
pulmonary circulation. J Appl Physiol 1990;69:237-44.
terial gas embolism, hyperbaric oxygen is the treat-
20. Spencer MP, Oyama Y. Pulmonary capacity for dissipation of venous gas emboli. Aerosp Med 1971;42:822-7.
ment of choice, as soon as cardiopulmonary stabili-
21. Tommasino C, Rizzardi R , Beretta L, Venturino M, Piccoli S. Cere-
bral ischemia after venous air embolism in the absence of intracardiac de-fects. J Neurosurg Anesthesiol 1996;8:30-4. REFERENCES 22. Katz J, Leiman BC, Butler BD. Effects of inhalation anaesthetics on filtration of venous gas emboli by the pulmonary vasculature. Br J Anaesth 1. Murphy BP, Harford FJ, Cramer FS. Cerebral air embolism resulting
from invasive medical procedures. Ann Surg 1985;201:242-5. 23. Ziser A, Adir Y, Lavon H, Shupak A. Hyperbaric oxygen therapy for
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
massive arterial air embolism during cardiac operations. J Thorac Cardio-
38. Thom SR , Mendiguren I, Hardy K, et al. Inhibition of human neu-
trophil beta2-integrin-dependent adherence by hyperbaric O2. Am J Phys-
24. Moon RE. Gas embolism. In: Oriani G, Marroni A, Wattel F, eds.
Handbook on hyperbaric medicine. Milan, Italy: Springer, 1996:229-48. 39. Dexter F, Hindman BJ. Recommendations for hyperbaric oxygen ther- 25. Dutka AJ. A review of the pathophysiology and potential application
apy of cerebral air embolism based on a mathematical model of bubble ab-
of experimental therapies for cerebral ischemia to the treatment of cerebral
sorption. Anesth Analg 1997;84:1203-7.
arterial gas embolism. Undersea Biomed Res 1985;12:403-21. 40. Peirce EC II. Specific therapy for arterial air embolism. Ann Thorac 26. Evans DE, Kobrine AI, Weathersby PK, Bradley ME. Cardiovascular
effects of cerebral air embolism. Stroke 1981;12:338-44. 41. Reasoner DK, Ryu KH, Hindman BJ, Cutkomp J, Smith T. Marked 27. Tovar EA, Del Campo C, Borsari A, Webb RP, Dell JR , Weinstein PB.
hemodilution increases neurologic injury after focal cerebral ischemia in
Postoperative management of cerebral air embolism: gas physiology for
surgeons. Ann Thorac Surg 1995;60:1138-42. 42. Ryu KH, Hindman BJ, Reasoner DK, Dexter F. Heparin reduces neu- 28. Voorhies RM, Fraser RAR. Cerebral air embolism occurring at angi-
rological impairment after cerebral arterial air embolism in the rabbit.
ography and diagnosed by computerized tomography. J Neurosurg 1984;
43. Kizer KW. Corticosteroids in treatment of serious decompression sick- 29. Smith RM, Van Hoesen KB, Neuman TS. Arterial gas embolism and
hemoconcentration. J Emerg Med 1994;12:147-53. 44. Ganshirt H. Significance of hemorheology in diagnosis and therapy of 30. Annane D, Troché G, Delisle F, et al. Effects of mechanical ventilation
ischemic cerebrovascular diseases: possibilities of therapy: antiedema pro-
with normobaric oxygen therapy on the rate of air removal from cerebral
cedures. Eur Neurol 1983;22:Suppl 1:78-82.
arteries. Crit Care Med 1994;22:851-7. 45. Sapolsky RM, Pulsinelli WA. Glucocorticoids potentiate ischemic in- 31. Workshop Panel. Final summary of recommendations: diving accident
jury to neurons: therapeutic implications. Science 1985;229:1397-400.
workshop 1990. In: Bennett PB, Moon RE, eds. Diving accident manage-
46. Dutka AJ, Mink RB, Pearson RR , Hallenbeck JM. Effects of treat-
ment. Bethesda, Md.: Undersea and Hyperbaric Medical Society, 1990:366-9.
ment with dexamethasone on recovery from experimental cerebral arterial
32. Moon RE, Dear GL, Stolp BW. Treatment of decompression illness
gas embolism. Undersea Biomed Res 1992;19:131-41.
and iatrogenic gas embolism. Respir Care Clin North Am 1999;5:93-135. 47. Evans DE, Kobrine AI, LeGrys DC, Bradley ME. Protective effect of 33. Bleck TP. Management approaches to prolonged seizures and status
lidocaine in acute cerebral ischemia induced by air embolism. J Neurosurg
epilepticus. Epilepsia 1999;40:Suppl 1:S59-S66. 34. Patel PM, Drummond JC, Cole DJ, Kelly PJ, Watson M. Isoflurane 48. Evans DE, Catron PW, McDermott JJ, Thomas LB, Kobrine AI,
and pentobarbital reduce the frequency of transient ischemic depolariza-
Flynn ET. Effect of lidocaine after experimental cerebral ischemia induced
tions during focal ischemia in rats. Anesth Analg 1998;86:773-80.
by air embolism. J Neurosurg 1989;70:97-102. 35. Hoffman WE, Charbel FT, Edelman G, Ausman JI. Thiopental and 49. Dutka AJ, Mink R , McDermott JJ, Clark JB, Hallenbeck JM. Effect
desflurane treatment for brain protection. Neurosurgery 1998;43:1050-3.
of lidocaine on somatosensory evoked response and cerebral blood flow af-
36. Miller JD, Ledingham IM, Jennett WB. Effects of hyperbaric oxygen
ter canine cerebral air embolism. Stroke 1992;23:1515-20.
on intracranial pressure and cerebral blood flow in experimental cerebral
50. McDermott JJ, Dutka AJ, Evans DE, Flynn ET. Treatment of experi-
oedema. J Neurol Neurosurg Psychiatry 1970;33:745-55.
mental cerebral air embolism with lidocaine and hyperbaric oxygen. Un-
37. Mink RB, Dutka AJ. Hyperbaric oxygen after global cerebral ischemia
in rabbits reduces brain vascular permeability and blood flow. Stroke 1995;
51. Mitchell SJ, Pellett O, Gorman DF. Cerebral protection by lidocaine
during cardiac operations. Ann Thorac Surg 1999;67:1117-24.
This is a general listing of accepted items. Please check your company’s plan documents for specific exclusions. For example, participation in a Health Savings Account would limit the reimbursable expenses listed below. To verify if a certain expense is covered if it is not listed below, please call 1-800-532-3327. This expense will qualify as long as the child qualifies as a tax dependent w
• The early days of the minipig • The reasons why minipigs came to be • Examples of safety pharmacology studies • Regulatory acceptability • For many years the standard approach has been to use a rodent and a non-rodent for safety assessments. – MICE: single & repeat dose studies, carcinogenicity. – RATS: single & repeat dose studies, reproductive – RABBITS: dermal stu
 The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Pathophysiology
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Pathophysiology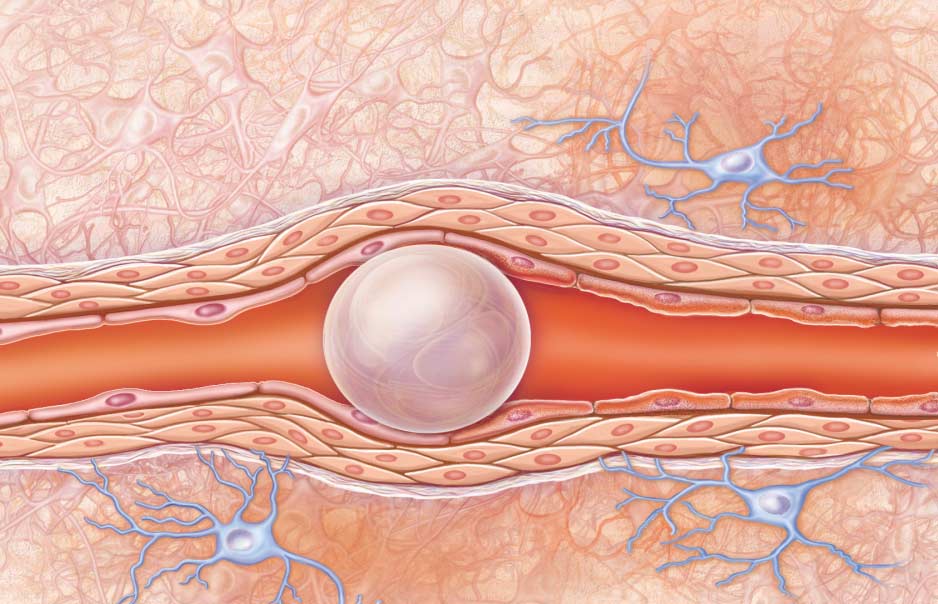
 P R I M A RY C A R E
P R I M A RY C A R E