I M P ROV E D S U RV I VA L W I T H R A D I OT H E R A PY A N D G O S E R E L I N I N LO CA L LY A DVA N C E D P RO STAT E CA N C E R IMPROVED SURVIVAL IN PATIENTS WITH LOCALLY ADVANCED PROSTATE CANCER TREATED WITH RADIOTHERAPY AND GOSERELIN
MICHEL BOLLA, M.D., DIONISIO GONZALEZ, M.D., PADRAIG WARDE, M.D., JEAN BERNARD DUBOIS, M.D.,
RENÉ-OLIVIER MIRIMANOFF, M.D., GUY STORME, M.D., JACQUES BERNIER, M.D., ABRAHAM KUTEN, M.D.,
CORA STERNBERG, M.D., THIERRY GIL, M.D., LAURENCE COLLETTE, M.SC., AND MARIANNE PIERART
ABSTRACT
ing to the tumor–node–metastasis [TNM] classifica-
Background
tion system of the International Union against Can-
spective trial comparing external irradiation with
cer). In a study begun in 1973, the overall survival
external irradiation plus goserelin (an agonist ana-
after 15 years for 287 patients with locally ad-
logue of gonadotropin-releasing hormone that re-
vanced prostate cancer who were treated with con-
duces testosterone secretion) in patients with locally
ventional external irradiation was 23 percent.3 Achiev-
ing local control after radiotherapy improved the
Methods
prognosis; among patients who did not have in-
cally advanced prostate cancer were randomly as-
volvement of regional lymph nodes at the time of
signed to receive radiotherapy alone or radiotherapy
diagnosis, 70 percent of those who attained local
plus immediate treatment with goserelin. The pa-tients had a median age of 71 years (range, 51 to 80).
control survived for 20 years free of distant metasta-
Patients in both groups received 50 Gy of radiation
ses, as compared with 13 percent of those who had
to the pelvis over a period of five weeks and an ad-
ditional 20 Gy over an additional two weeks as a
Hormonal therapy often prolongs the suppression
prostatic boost. Patients in the combined-treatment
of the primary tumor by radiotherapy,5 but the
group received 3.6 mg of goserelin (Zoladex) subcu-
question remains whether hormonal therapy should
taneously every four weeks starting on the first day
be reserved for relapse or used early in asymptomatic
of irradiation and continuing for three years; those
patients with locally advanced disease who are receiv-
patients also received cyproterone acetate (150 mg
ing external radiation treatment. Three controlled
orally per day) during the first month of treatment to
clinical trials have failed to demonstrate the value of
inhibit the transient rise in testosterone associatedwith the administration of goserelin.
prophylactic therapy with diethylstilbestrol, orchi-
Results
ectomy, or both in patients treated with external
patients. The median follow-up was 45 months. Kap-
radiotherapy.6-8 A study of 277 patients found no
lan–Meier estimates of overall survival at five years
differences among those undergoing orchiectomy,
were 79 percent (95 percent confidence interval, 72
radiotherapy, or combined treatment; orchiectomy,
to 86 percent) in the combined-treatment group and
however, whether alone or combined with radio-
62 percent (95 percent confidence interval, 52 to 72
therapy, significantly delayed metastases as compared
percent) in the radiotherapy group (Pϭ0.001). The
proportion of surviving patients who were free of
Goserelin is an agonist analogue of gonadotropin-
disease at five years was 85 percent (95 percent con-
releasing hormone that induces hypogonadism by
fidence interval, 78 to 92 percent) in the combined-
reducing the secretion of gonadotropin and there-
treatment group and 48 percent (95 percent confi-dence interval, 38 to 58 percent) in the radiotherapy
fore testosterone. The purpose of this trial was to
determine whether treatment with goserelin, when
Conclusions
initiated during the first week of irradiation, increas-
when started simultaneously with external irradia-
es disease-free survival and prolongs overall survival
tion, improves local control and survival in patients
in patients at high risk for metastatic prostate cancer.
with locally advanced prostate cancer. (N Engl J Med1997;337:295-300.)1997, Massachusetts Medical Society.
From University Hospital, Grenoble, France (M.B.); Akademisch Me-
disch Centrum, Amsterdam, the Netherlands (D.G.); Princess Margaret
HE role of external irradiation in patients
Hospital, Toronto (P.W.); Centre Régional de Lutte contre le Cancer Val
d’Aurelle, Montpellier, France (J.B.D.); Centre Hospitalier UniversitaireVaudois, Lausanne, Switzerland (R.-O.M.); Oncologisch Centrum, Brus-
controversial.1,2 At this stage of the disease
sels (G.S.); Ospedale San Giovanni, Bellinzona, Switzerland (J.B.); Ram-
bam Medical Center, Haifa, Israel (A.K.); Ufficio Sternberg & Pansadoro,Rome (C.S.); and the European Organization for Research and Treatment
the prostate; it may infiltrate neighboring structures
of Cancer Data Center, Brussels (T.G., L.C., M.P.). Address reprint re-
and involve regional lymph nodes, but there are no
quests to Dr. Bolla at the Radiotherapy Department, University Hospital,
distant metastases (stage T3–4, N0–2, M0, accord-
B.P. 217 38043 Grenoble CEDEX 9, France.
Downloaded from www.nejm.org on June 1, 2009 . For personal use only. No other uses without permission.
Copyright 1997 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
sient symptoms; 2, distressing, persistent, or recurring symptomsrequiring occasional prolonged medical treatment; 3, symptoms
Eligibility Criteria
requiring prolonged medical treatment, surgical intervention, or
Patients were eligible if they were under 80 years of age, with
both; or 4, fatal complications. For patients receiving goserelin,
histologically proved prostatic adenocarcinoma that was intracap-
adverse reactions were registered as hot flashes and gynecomastia.
sular (T1) or confined to the gland (T2), without detectable in-
volvement of regional lymph nodes (N0-X), and of World HealthOrganization (WHO) histologic grade 3; or if they had prostate
Assessment of Progression
cancer of any histologic grade that extended beyond the capsule
Local failure was defined as an increase of more than 50 per-
(T3) or infiltrated neighboring structures (T4) without involving
cent in the product of the two maximal perpendicular diameters
regional lymph nodes. The clinical evaluation included bone
of the primary lesion as measured digitally, by CT or transabdom-
scanning, chest radiography, and ultrasonography or computed
inal ultrasonography; in case of doubt, biopsy was highly recom-
tomography (CT) of the liver. Lymph nodes were evaluated by
mended. Local progression was defined as the recurrence of a pal-
CT, bipedal lymphangiography, or extraperitoneal lymphadenec-
pable tumor after initial regression. Regional failure, in the pelvic
tomy. Laboratory studies included complete blood counts and
or paraaortic lymph-node areas, was demonstrated by ultrasonog-
measurements of creatinine, serum prostatic acid phosphatase, se-
raphy or CT and was confirmed by biopsy. Distant metastases in
rum testosterone, and prostate-specific antigen (PSA), as assessed
bones, parenchymal organs, or soft tissues were identified radio-
by radioimmunometric or immunoenzyme assays. Eligible patients
logically and then by biopsy if deemed necessary.
had had no previous treatment for prostate cancer and gave writ-ten informed consent. Patients with a previous malignant disease,
Quality Assurance
except for treated basal-cell carcinoma of the skin, and those withevidence of distant metastases, including metastases to common
The calibration of every linear accelerator was obtained by
iliac or paraaortic lymph nodes, were excluded. Pathological spec-
mailed thermoluminescence dosimetry checks. Individual clinical,
biologic, pathological, and follow-up procedures for the mainparticipating centers were reviewed individually to reconcile dis-
Techniques of Treatment
crepancies between local data and data registered at the EuropeanOrganization for Research and Treatment of Cancer (EORTC)
Radiotherapy
Data Center. Protocol compliance was checked by a dummy-runprocedure to evaluate differences in the definition of target vol-
Photons of 10 MV and above were recommended; when they
ume, in treatment technique, and in dose specification and ho-
were not available, the use of cobalt-60 was acceptable provided
the skin-to-source distance was more than 80 cm and patientshad a maximal anterior–posterior pelvic diameter of less than 22cm. Planning target volume I was the whole pelvis, and planning
End Points and Statistical Analysis
target volume II the prostate and seminal vesicles. The whole pel-
Overall survival was measured from the date of randomization
vis was irradiated with a four-field technique, with one anterior–
to the date of death or the most recent follow-up. The disease-
posterior field, one posterior–anterior field, and two parallel op-
free interval was measured from the date of randomization to the
posed lateral fields. In the craniocaudal direction the upper limit
date of local or regional failure, the first appearance of distant me-
was the L5–S1 interspace, the lower limit was the ischial tuberos-
tastases, or the last follow-up, whichever occurred first. The time
ities, and the lateral margins were 1 cm beyond the maximal width
until the first treatment failure after a biologic response was meas-
of the bony pelvis; some centers preferred to irradiate a smaller tar-
ured from the date of randomization to the date of clinically de-
get volume by using anterior–posterior fields averaging 12 by 12
termined progression, PSA-determined progression, or the most
cm and lateral fields averaging 12 by 10 cm. Planning target vol-
recent follow-up; PSA-determined progression was defined as a
ume II was irradiated with either the same technique or with three
PSA level greater than 1.5 ng per milliliter and increasing on two
fields: one anterior–posterior and two lateral fields with wedge fil-
ters. The anterior and posterior security margins on the lateral
The protocol was designed to detect a minimal increase from
fields were at least 2 cm. The specification of the dose was given
40 percent to 55 percent in the 5-year disease-free rate, corre-
at the intersection of the beam axes according to Report 29 of the
sponding to an increase from 3.8 to 5.8 years in the median dis-
International Commission on Radiation Units and Measurements.10
ease-free interval (assuming exponential distribution). To detect
The dose per fraction was 2 Gy. Patients were treated once a day,
this difference, 75 patients in each treatment group had to be fol-
five days a week, for seven weeks; planning target volume I was ir-
lowed until relapse (aϭ0.05, bϭ0.2). Survival curves were esti-
radiated during a five-week period with up to 50 Gy, and planning
mated by using the Kaplan–Meier technique.13 All comparisons
target volume II was treated during the last two weeks with an ad-
were made by means of a two-sided log-rank test with a 0.05 sig-
nificance level.14 Data were analyzed according to the intention-to-treat principle. Hormonal Treatment
Goserelin (Zoladex, Zeneca-Pharma) was supplied by the man-
Randomization
ufacturer in a disposable syringe loaded with 3.6 mg of the drug
Randomization was centralized at the EORTC Data Center.
and fitted with a 16-gauge needle. The drug was administered
Patients were stratified according to institution, the clinical stage
subcutaneously every four weeks, starting on the first day of pel-
of the disease, the results of extraperitoneal pelvic lymph-node bi-
vic irradiation and continuing for three years; 150 mg of a steroi-
opsy, and the irradiation technique. The randomization was per-
dal antiandrogen, cyproterone acetate (Androcur, Schering), was
given orally for one month, starting one week before the firstdose of goserelin, to inhibit the transient rise of testosterone
Characteristics of the Patients Toxicity
From May 1987 through September 1995, 415
Acute side effects of radiotherapy were scored according to the
WHO scale.11 Late toxicity was scored according to the Radio-
patients entered the study — 208 in the pelvic-
therapy Oncology Group scale: 0, no symptoms; 1, minor tran-
radiotherapy group and 207 in the combined-treat-
Downloaded from www.nejm.org on June 1, 2009 . For personal use only. No other uses without permission.
Copyright 1997 Massachusetts Medical Society. All rights reserved.
I M P ROV E D S U RV I VA L W I T H R A D I OT H E R A PY A N D G O S E R E L I N I N LO CA L LY A DVA N C E D P RO STAT E CA N C E R
ment group. The median duration of follow-up was45 months. At the time of analysis, all but 14 pa-
TABLE 1. AGE, PERFORMANCE STATUS, WHO GRADE,
tients had been evaluated. For the analysis, these 14
patients were considered eligible. Ten patients — six
in the radiotherapy group and four in the com-bined-treatment group — were ineligible because ofbone metastases (two patients), paraaortic lymph-
COMBINED RADIOTHERAPY TREATMENT
node metastases (one), thrombocytopenia (one), in-
CHARACTERISTIC* (N؍198) (N؍203)
appropriate clinical stages (T1G1, one; T2G1, one;
and T2G2, three; and T2 without mention of grade,
one). The two groups of patients were well balanced
with regard to age, WHO performance status, clini-
cal stage, presence or absence of pelvic lymph-nodemetastases, WHO histologic grade, Gleason grade,
serum acid phosphatase level, and base-line PSA lev-
el (Table 1). Cardiovascular disease was present in
29 percent of the patients in the radiotherapy group
and 24 percent of those in the combined-treatment
group; no chronic disease was mentioned for 48
percent of the patients in the radiotherapy group as
compared with 53 percent in the combined-treat-
Compliance
Information about treatment was available for
401 patients — 198 in the radiotherapy group and
203 in the combined-treatment group. Of the pa-
tients in the radiotherapy group, 99 percent re-
ceived external irradiation; 80 percent of these pa-
tients received large-field and 20 percent small-field
radiotherapy. Three of the 198 patients refused the
Of the 203 patients in the combined-treatment
group, 2 refused any treatment and 6 refused hor-
monal therapy. At the time of analysis, not all the pa-
tients in this group had completed the three-year
treatment with goserelin, but 15 patients continued
that treatment for more than three years (Table 2).
Eighty-one percent of the patients in this group re-
*T denotes tumor and N node, according to the TNM
ceived large-field and 19 percent small-field radio-
(tumor–node–metastasis) classification system; PSA denotes
Toxicity
Of the acute toxic effects listed in Table 3, none
with a grade of 3 or 4 affected more than 5 percent
grade 1–3 urethral stricture (20 percent in the com-
of either group except for diarrhea. With a median
bined-treatment group vs. 13 percent in the radio-
follow-up of 45 months, not more than 1 percent
therapy group) were not significantly different (Pϭ
of either group had grade 3 late toxic effects, in-
0.09). Thirty-eight patients (19 percent) had adverse
cluding hematuria, chronic diarrhea, proctitis, cysti-
reactions to the gonadotropin-releasing hormone
tis, small-bowel obstruction, incontinence, and ure-
analogue: hot flashes (22 patients), gynecomastia
thral stricture. Data on erectile function were not
(4), mastodynia (1), breast pain and galactorrhea
collected systematically. Among the patients receiv-
(1), sweating (2), weakness (2), depression (1),
ing goserelin, 62 percent had hot flashes, but only
deep venous thrombosis (1), and unspecified reac-
34 percent had more than three per day. During
follow-up, more patients in the combined-treat-ment group than in the radiotherapy group had late
Efficacy
grade 1–3 incontinence (29 percent vs. 16 percent,
The Kaplan–Meier estimate of overall survival at
Pϭ0.002); the proportions of patients with late
five years in the combined-treatment group was 79
Downloaded from www.nejm.org on June 1, 2009 . For personal use only. No other uses without permission.
Copyright 1997 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
treatment group. Of these deaths, 26 in the radio-
TABLE 2. COMPLIANCE WITH THE
therapy group and 6 in the combined-treatment
group were due to prostate cancer. Among the pa-
tients who survived for five years, the disease-freerate was 85 percent (95 percent confidence interval,
COMPLIANCE
78 to 92 percent) in the combined-treatment group
and 48 percent (95 percent confidence interval, 38
to 58 percent) in the radiotherapy group (hazard
ratioϭ0.22; 95 percent confidence interval, 0.15
to 0.32; PϽ0.001) (Fig. 2). Seventy-eight patients
had disease progression in the radiotherapy group,
as compared with 20 in the combined-treatment
group. Table 4 shows the sites of progression. In theradiotherapy group, the treatment given after pro-
*Five patients declined further treatment because
gression included goserelin in 56 cases (72 percent)
of hot flashes (after 3, 8, 11, 14, and 16 months). Two patients had their treatment stopped because of
and another hormonal treatment in 17 cases and
depression (after 3 and 19 months). One patient
was unspecified in 5 cases. The 17 other treatments
stopped because of mastodynia and galactorrhea (af-
were orchiectomy (eight patients), another hormo-
nal treatment (two), delayed treatment (five), and
†One patient underwent orchiectomy because of
poor compliance with goserelin treatment (after 20
no treatment, because of intercurrent death (one)
months). One patient stopped taking goserelin to
and the patient’s refusal (one). The five-year local-
undergo urethrotomy because of recurrent strictures
control rate was 97 percent in the combined-treat-
(after 4 months). One patient was lost to follow-up(after 15 months). Two patients stopped the radio-
ment group and 77 percent in the radiotherapy
therapy and goserelin treatment for reasons unrelat-
group (hazard ratioϭ0.19; 95 percent confidence
ed to the potential side effects of the drug.
interval, 0.10 to 0.37; PϽ0.001). The combined-treatment group had a longer time until the firsttreatment failure after a biologic response than theradiotherapy group (6.6 years [95 percent confi-dence interval, 3.5 to 5.3] vs. 4.4 years [95 percent
TABLE 3. GRADE 3 OR 4 TOXIC EFFECTS
confidence interval, 5.8 to 9.0]; hazard ratio
95 percent confidence interval, 0.11 to 0.48; PϽ
0.001). The five-year failure-free rate after biologicresponse was 81 percent for the combined-treat-
COMBINED
ment group and 43 percent for the radiotherapy
RADIOTHERAPY TREATMENT TOXIC EFFECT (N؍195) (N؍201) DISCUSSION
We found that adjuvant therapy with an analogue
of gonadotropin-releasing hormone (goserelin), start-
ed at the beginning of external irradiation treatment
and continuing for three years, can improve the five-
year overall survival of patients with locally advanced
prostate cancer. Two previous studies have compared
short-term hormonal therapy before and during ex-
ternal irradiation, or long-term hormonal therapy af-
ter external irradiation, with radiation therapy alone
for locally advanced prostatic carcinoma. The hor-
*Only grade 3 toxic effects were observed.
monal therapy included flutamide and goserelin forthe former and goserelin alone for the latter; bothprotocols showed advantages over radiotherapy alonein terms of local control, the incidence of distant
percent (95 percent confidence interval, 72 to 86
metastases, and progression-free survival.16,17 How-
percent), as compared with 62 percent (95 percent
ever, it is difficult to compare these three trials, since
confidence interval, 52 to 72 percent) in the radio-
the eligibility criteria, the timing and duration of ad-
therapy group (Pϭ0.001) (Fig. 1). For overall sur-
ministration of goserelin, the definition of local con-
vival, the hazard ratio was 0.50 (95 percent confi-
trol, and the results in the radiotherapy groups are
dence interval, 0.33 to 0.76). There were 58 deaths
not quite comparable. In our study, we assessed lo-
in the radiotherapy group and 35 in the combined-
cal control by endorectal examination; a second bi-
Downloaded from www.nejm.org on June 1, 2009 . For personal use only. No other uses without permission.
Copyright 1997 Massachusetts Medical Society. All rights reserved.
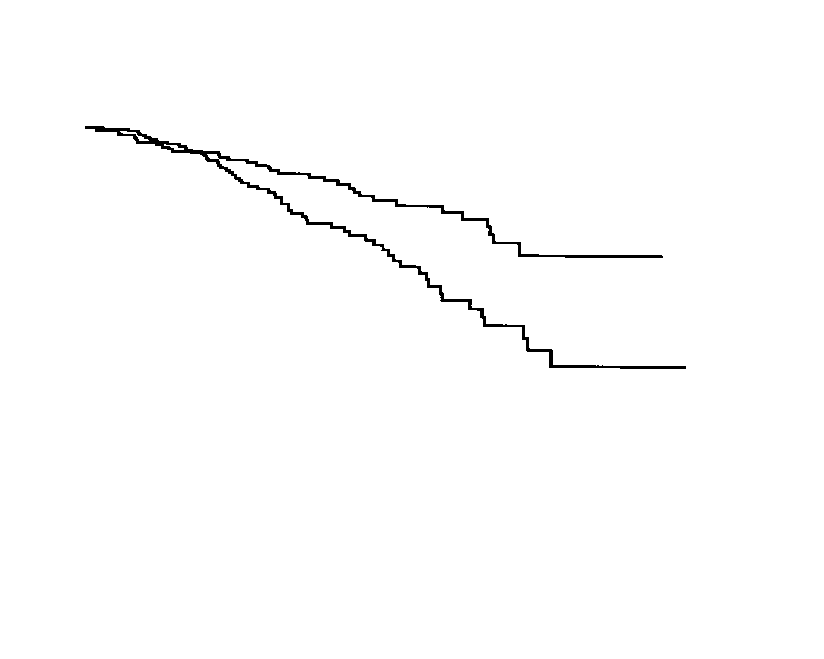
I M P ROV E D S U RV I VA L W I T H R A D I OT H E R A PY A N D G O S E R E L I N I N LO CA L LY A DVA N C E D P RO STAT E CA N C E R Figure 1. Kaplan–Meier Estimate of Overall Survival.
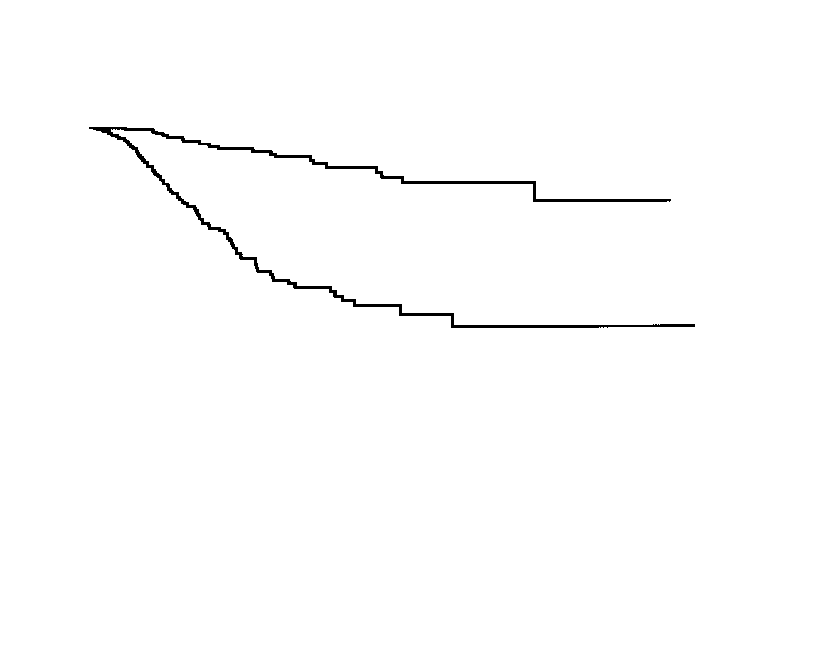
The overall survival rate at five years was 79 percent (95 percent confidence interval,72 to 86 percent) for the combined-treatment group and 62 percent (95 percent con-fidence interval, 52 to 72 percent) for the group treated only with radiotherapy. Figure 2. Kaplan–Meier Estimate of the Disease-free Interval.
This curve shows the proportion of surviving patients who were free of disease ateach time point. The method takes the censoring process into account. The numberof patients who are at risk for the event at each time point is the total number of pa-tients minus the number in whom disease progressed or who were lost to follow-up.
opsy of the prostate was not mandatory if the endo-
French institutes from 1983 to 1987. The rate of lo-
rectal examination was normal, even if the serum
cal control at five years was 79 percent, as compared
PSA level was elevated. This aspect of assessment has
with 77 percent (95 percent confidence interval, 68
been addressed previously, and one year after the
to 86 percent) in the EORTC trial.19 The time until
completion of external irradiation the rate of posi-
the first treatment failure after a biologic response is
tive biopsy results has been found to reach a plateau
a surrogate end point that represents the time from
of 35 percent.18 The clinical results in our control
randomization to the date of clinically determined
group are in keeping with those of a retrospective
progression or PSA-determined progression. Analysis
analysis of 397 patients, with stage T3–T4 disease,
using this end point showed a significant difference
who were treated only by external irradiation in 19
between combined treatment and radiotherapy alone
Downloaded from www.nejm.org on June 1, 2009 . For personal use only. No other uses without permission.
Copyright 1997 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
REFERENCES TABLE 4. SITES OF DISEASE PROGRESSION. 1. Bagshaw MA, Cox RS, Ray GR. Status of radiation treatment of pros- tate cancer at Stanford University. In: Consensus Development Conference on the Management of Clinically Localized Prostate Cancer. National Can- COMBINED
cer Institute monographs. No. 7. Washington, D.C.: Government Printing
TYPE OF PROGRESSION TREATMENT
Office, 1988:47-60. 2. National Institutes of Health Consensus Development Panel. Consen-
sus statement: the management of clinically localized prostate cancer. In: Consensus Development Conference on the Management of Clinically Lo-
calized Prostate Cancer. National Cancer Institute monographs. No. 7.
Washington, D.C.: Government Printing Office, 1988:3-6. 3. Hanks GE, Corn BW, Lee WR, Hunt M, Hanlon A, Schultheiss TE.
External beam irradiation of prostate cancer: conformal treatment tech-niques and outcomes for the 1990s. Cancer 1995;75:1972-7. 4. Leibel SA, Fuks Z, Zelefsky MJ, Whitmore WF Jr. The effects of local and
regional treatment on the metastatic outcome in prostatic carcinoma with
pelvic lymph node involvement. Int J Radiat Oncol Biol Phys 1994;28:7-16. 5. Schröder FH. What is new in endocrine therapy of prostatic cancer? In: Newling DWW, Jones WG, eds. EORTC Genitourinary Group monograph 7. Prostate cancer and testicular cancer. New York: Wiley–Liss, 1990:45-52. 6. van der Werf-Messing B, Sourek-Zikova V, Blonk DI. Localized ad- vanced carcinoma of the prostate: radiation therapy versus hormonal ther-
(hazard ratioϭ0.17; 95 percent confidence interval,
apy. Int J Radiat Oncol Biol Phys 1976;1:1043-8. 7. Neglia WJ, Hussey DH, Johnson DE. Megavoltage radiation therapy for
carcinoma of the prostate. Int J Radiat Oncol Biol Phys 1977;2:873-83. 8. Taylor WJ, Richardson RG, Hafermann MD. Radiation therapy for lo- calized prostate cancer. Cancer 1979;43:1123-7. 9. Fellows GJ, Clark PB, Beynon LL, et al. Treatment of advanced loca- We are indebted to Zeneca-Pharma for providing Zoladex and to
lised prostatic cancer by orchiectomy, radiotherapy, or combined treat-ment: a Medical Research Council study. Br J Urol 1992;70:304-9. F.W.J. Ten Kate, M.D., J. Mattelaer, M.D., J. Lopez Torrecilla,10. ICRU report 29. Dose specification for reporting external beam ther- M.D., J.R. Pfeffer, M.D., C.L. Cutajar, M.D., T. Roberts, M.D.,
apy with photons and electrons. Washington, D.C.: International Commis-
S. Fossa, M.D., J.C. Horiot, M.D., H. Hamers, M.D., J.F. Bossett,
sion on Radiation Units and Measurements, April 1, 1978. M.D., F. Kovner, M.D., H. Van Poppel, M.D., J. Jager, M.D., V. Svo-11. WHO handbook for reporting results of cancer treatment. Geneva: boda, M.D., J.J. Zambon, M.D., J.J. Wijndaele, M.D., O. Koriakine,M.D., and C. Boekenkruger, M.D., for their collaboration.12. Dusserre A, Garavaglia G, Giraud JY, Bolla M. Quality assurance of the EORTC radiotherapy trial 22863 for prostatic cancer: the dummy run. Radiother Oncol 1995;36:229-34. APPENDIX 13. Kaplan EL, Meier P. Nonparametric estimation from incomplete ob- servations. J Am Stat Assoc 1958;53:457-81.
The following EORTC Radiotherapy Cooperative Group in-
14. Mantel N. Evaluation of survival data and two new rank order statistics
stitutions participated in this study: Grenoble, Hôpital Albert
arising in its consideration. Cancer Chemother Rep 1966;50:163-70.
Michallon; Montpellier, Centre Val d’Aurelle; Dijon, Centre
15. Pocock SJ, Simon R. Sequential treatment assignment with balancing for
Georges-François Leclerc; Besançon, Hôpital Jean Minjoz; Am-
prognostic factors in the controlled clinical trial. Biometrics 1975;31:103-15.
sterdam, Akademisch Medisch Centrum; Heerlen, Radiotherapeu-
16. Pilepich MV, Krall JM, al-Sarraf M, et al. Androgen deprivation with
tisch Instituut Limburg; Tilburg, B. Verbeeten Instituut; Lausanne,
radiation therapy compared with radiation therapy alone for locally ad-
Centre Hospitalier Universitaire Vaudois; Bellinzona, Ospedale
vanced prostatic carcinoma: a randomized comparative trial of the Radia-
San Giovanni; Toronto, Princess Margaret Hospital; Haifa, Ram-
tion Therapy Oncology Group. Urology 1995;45:616-23. 17. Pilepich MV, Caplan R, Byhardt RW, et al. Phase III trial of androgen
bam Medical Hospital; Jerusalem, Hadassah University Hospital;
suppression using goserelin in unfavorable-prognosis carcinoma of the
Tel Aviv, Tel Aviv Medical Center–Ichilov Hospital; Valencia, In-
prostate treated with definitive radiotherapy. Prog Proc Am Soc Clin Oncol
stituto Valenciano de Oncologia; and Portsmouth, St. Mary’s
18. Scardino PT, Wheeler TM. Local control of prostate cancer with ra-
The following EORTC Genitourinary Group institutions par-
diotherapy: frequency and prognostic significance of positive results of
ticipated in this study: Maastricht, Akademisch Ziekenhuis; Rot-
postirradiation prostate biopsy. In: Consensus Development Conference
terdam, Zuiderziekenhuis; Brussels, Akademisch Ziekenhuis; Kort-
on the Management of Clinically Localized Prostate Cancer. National Can-
rijk, St. Maarten Hospital; Leuven, Universitair Ziekenhuis Sint
cer Institute monographs. No. 7. Washington, D.C.: Government Printing Office, 1988:95-103.
Rafael; Antwerp, Universitair Ziekenhuis; Rome, Ufficio Stern-
19. Rozan R, Albuisson E, Kin B, et al. External beam radiation of stage
berg & Pansadoro; Malta, St. Luke’s Hospital; Newcastle-upon-
T3/T4 adenocarcinoma of the prostate. In: Bolla M, Rambeaud JJ, Vin-
Tyne, Freeman Hospital; Obninsk, Medical Radiological Re-
cent F, eds. Local prostatic carcinoma. Basel, Switzerland: Karger, 1994:
search Center; and Oslo, Norwegian Radium Hospital.
Downloaded from www.nejm.org on June 1, 2009 . For personal use only. No other uses without permission.
Copyright 1997 Massachusetts Medical Society. All rights reserved.
Texas Health Care, P.L.L.C. Colon & Rectal SurgeryBritton R. West, M.D., Stephen D. Fitzgerald, M.D., Glen D. Hooker, M.D., Eduardo D. Castillo, M.D. 1420 8th Avenue, Suite 103, Fort Worth, Texas 76104 BEFORE ANORECTAL SURGERY 1. Extra fiber intake 2 days before surgery and 2 weeks after surgery helps to prevent constipation. Take 2 tablespoons or 2tablets of fiber (Citrucel, Metamucil,
Was Sie selbst tun sollten Was Partner tun können Gehen Sie zunächst zum Hausarzt – er wird die grundlegenden Seien Sie verständnisvoll und geben Sie Mut. Faktoren abklären und Sie bei Bedarf zum Urologen überweisen. Üben Sie keinen Druck aus, haben Sie Scheuen Sie nicht den Weg zum Urologen; nehmen Sie dort Partner, einen Arzt ins Vertrauen zu ziehen. Zi
 I M P ROV E D S U RV I VA L W I T H R A D I OT H E R A PY A N D G O S E R E L I N I N LO CA L LY A DVA N C E D P RO STAT E CA N C E R
I M P ROV E D S U RV I VA L W I T H R A D I OT H E R A PY A N D G O S E R E L I N I N LO CA L LY A DVA N C E D P RO STAT E CA N C E R