HEALTH PROTECTION AGENCY NORTH WEST The Management of Scabies infection in the Community
There are other national guidelines available.
This is recommended for use in the North West.
Steve Gee, Ed Kaczmarski, Jeanette Kempster
Lorraine Lighton, Gill Marsh, Ken Mutton, Ruth Philp and Jeff Scott
on behalf of the North West Policy Group
Health and Social Care Settings (e.g. Care Homes, Day Centres)
Principles of outbreak management and control
Appendix One Residents diagnosed with a scabies rash
Appendix Two Staff diagnosed with a scabies rash
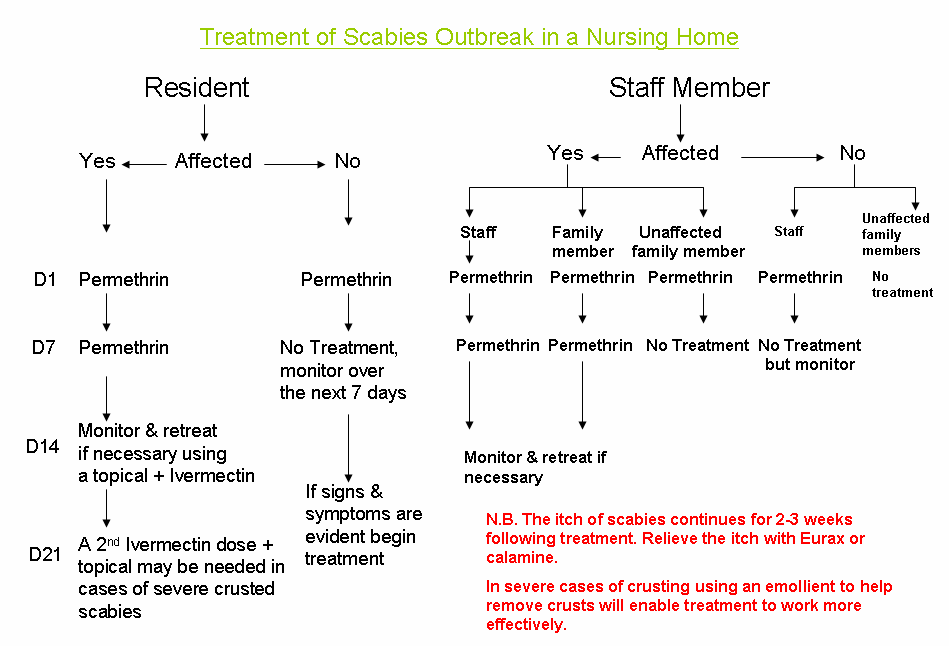
Appendix Five Treatment of scabies outbreaks in care homes
Thanks to Peter Morgan, Ashton, Leigh & Wigan Community Services.
Introduction
Scabies is a contagious infection caused by a mite Sarcoptes scabiae var.hominis. The condition is recognised by an allergic reaction to the saliva & faecal material excreted by the mite. It is a worldwide disease, more common where overcrowded conditions prevail. It can affect any individual irrespective of social class or race. It is primarily characterised by itching and vesiculations. Signs of reddish, slightly elevated tracts may also occur. Miniature papules, vesiculations, pustules and excoriations soon appear. Scratching of these areas may lead to secondary bacterial infection, sometimes requiring antimicrobial treatment.
Mode of Transmission
Scabies is host specific i.e. Sarcoptes scabiae var.hominis only lives on humans, therefore scabies cannot be caught from pets or other animals. Transmission is by direct personal contact i.e. by prolonged skin-to-skin contact of a sexual or social nature, and thus a quick handshake or hug will not spread the infection. Mites usually pass from person-to-person in close communities, particularly within households. It is recognised that the spread is not limited to family members, but includes everyone who has intimate personal contact with infected individuals. Infection occurs following transference of mites, which burrow into the skin. People who have acquired the infection for the first time may not show any symptoms for 2 - 4 weeks, so this makes spread of the disease difficult to identify and contain in institutions such as care homes.
Life Cycle of the Mite
• The newly mated female burrows through the skin, often at the finger webs, wrists and
• Eggs are laid in the burrows at a rate of 2 - 3 per day for up to 2 months.
• Eggs mature, and larvae emerge from the eggs 3-4 days after they have been laid.
• After emerging from the egg, the larva passes through two moults before becoming
• The entire life cycle can be completed in 10-14 days, and mites live for around 30 days.
Incubation Period
The incubation period for a first infection is usually 2 - 4 weeks in people without previous exposure, as the mites faecal contamination takes time to cause an allergic reaction. Subsequent infection will cause an allergic reaction within one week. Scabies can be easily managed when treatment is performed correctly. However, as a result of the extended incubation period there may also be asymptomatic carriers who can re-infect others after treatment has been performed. It is therefore important to undertake a thorough risk assessment when planning eradication treatment and to undertake follow up skin assessments for at least two weeks post treatment (see Section 14 of this document).
Sites of Infection
The most common areas affected are between the fingers (finger webs), wrists, elbows, armpits, waist, thighs, genitalia, nipples, breasts and lower buttocks. In infants, young children the elderly and those who are chronically ill, the mites can be found on the face, ears and scalp (figure 1). It should be recognised that scabies causes an allergic reaction, and the itch and the rash may not always coincide with the actual site of the mite.
Recognition/Diagnosis
Appropriately trained professionals who will look for burrows and/or mites can make a clinical diagnosis. Usually there are only a few mites on the entire body and therefore evidence of infection can easily be missed. Recovering the mite from its burrow by taking skin scrapings and identifying it microscopically may establish diagnosis. However scabies should always be suspected in the presence of the following symptoms:
• intense itching, particularly at night
• burrows and other lesions on the sites mentioned above
The rash is a symmetrical itchy red papular rash which is an allergic reaction of the body to the saliva & faeces of the mite, and the eggs deposited by the mite under the skin. The allergic reaction may not correspond with the site where the mite may actually be found. The appearance and severity of symptoms varies from person to person and as with all allergies, the symptoms and their severity are strongly influenced by the immune status of the affected individuals.
Classification of Scabies
There are two classes of scabies infection; both are caused by the same mite.
Classical scabies
• Found in people with normal immune systems.
• Itch can start between 2 - 4 weeks following initial acquisition of the infection.
• Sites of the rash may not correspond to sites of the mites.
8.2 Hyperkeratotic Scabies
(also known as crusted, Norwegian and atypical scabies)
• An unusual form of the infection that is highly contagious.
• Occurs in immunodeficient individuals e.g. the frail elderly.
• Infection often appears as a generalized dermatitis more widely distributed than the
burrows and the usual severe itching may be reduced or absent.
• Persons with crusted scabies are highly contagious because of the large number of
• Skin becomes thickened, scaled, crusted and unsightly due to the numbers of mites
Contact Tracing
Unless the original source of infection and all contacts are identified and treated, the disease will continue to spread with the possibility of re-infection for those already treated. The purpose of contact tracing is to identify anyone who may be infected and advise them about treatment options. All those with who intimate skin contact was made for a prolonged period of time within the previous 2-6 weeks must be identified. It is beneficial for those people to seek information and guidance from their family doctor, practice nurse, community pharmacist or where appropriate their occupational health department.
10. Treatment
The index case (first person identified as having Scabies) and all members of the affected household should be treated simultaneously even in the absence of symptoms. It is also important to stress that this is not limited to family members but should include everyone who has had intimate contact with infected affected individuals, e.g. sexual contacts. All members of the household should be treated at the same time (preferably within twenty four hours). For those who have been diagnosed with a scabies rash, treatment should be undertaken twice, one week apart.
11. Scabicidal treatments for topical use
In symptomatic persons it is recommended that these products be applied twice, seven days apart. Aqueous liquids and dermal creams are preferable to alcoholic preparations; they are easier to apply and are less irritating to the sensitive areas of the skin.
A non-pyrethroid product should be recommended for people who are allergic to Chrysanthemums.
Not contra-indicated in pregnancy or breast-feeding.
Transmission of the mite ceases after the first application has been applied, however, itching may persist for some time following successful treatment.
Use sufficient quantities of the scabicide, usually 30 grammes = 1 tube of cream or 100mls of lotion, this will cover the average person, but larger people in size and body weight will require two tubes of cream/bottles of lotion to ensure all areas of the body are covered adequately.
11.1 Permethrin 5% Dermal Cream (pyrethroid)
• Should be applied to the whole body including the face, neck, scalp & ears.
• It should be washed off after eight - twelve hours contact time.
• If hands (or other areas of the body) are washed within the eight - twelve hours
application period, reapply to that area of the skin.
• Children aged 2 months to two years medical supervision is required.
• Do not apply to broken or secondarily infected skin.
11.2 Malathion 0.5% Liquid (organo-phosphate)
• Should be applied to the whole body including face, neck, scalp & ears.
• It should be washed off after 24 hours contact time.
• If hands (or other areas of the body) are washed within the 24 hours of application,
• For young children under 6 months, use under medical supervision.
• Do not apply to broken or secondarily infected skin. 11.3 Benzyl Benzoate B.P
The use of Benzyl Benzoate as a treatment for scabies infection is generally no longer recommended, as it has been superseded by more contemporary products (see 11.1 & 11.2). It requires a long contact time (24 hours) with a repeat application after 24 hours (sometimes a third application is required) without the patient bathing in between applications. It is not recommended for use in children, should not be applied to broken or secondarily infected skin, and should not be used be used by breast-feeding mothers.
12. Treatment of classical scabies
Aqueous liquid or dermal cream should be applied by rubbing gently onto all parts of the body including the face, neck, behind the ears and the scalp. Hot baths before treatment should be avoided as evidence suggests this aids absorption into the blood stream, and reduces its action at the site.
The liquid or cream should be allowed to dry before getting dressed.
Partners and close contacts should be treated simultaneously (within 24 hours).
People may need assistance to apply the treatment properly and special attention should be paid to armpits, wrists, elbows, finger webs and under nails, beneath the breasts and around the nipples, the soles of the feet and the toes. Liquid should be brushed under the ends of the nails.
The cream or liquid should be reapplied after washing hands or other areas of the skin (e.g. after nappy changing or after a person is incontinent) during the treatment time, and, to prevent small children and babies sucking the treatment from their hands, mittens can be worn.
There is no evidence to suggest that scabies is transmitted on clothing, towels and bedding, therefore no special cleaning or laundering measures other than the usual hygienic ones are required following treatment.
People should be advised that itching could persist for some time after successful treatment. An anti-pruritic (itching) cream may be helpful. However, persistent symptoms for more than 2 weeks may indicate that the eradication treatment has not been successful, and may indicate that a further risk assessment (see Section 14 of this document) &/or treatment is required
The guiding principle is co-ordination of treatment to limit both spread of the disease and unnecessary scabicidal exposure. Successful treatment does not however protect the person from re-infection from undiagnosed contacts inside and outside the family / household.
13. Treatment of hyperkeratotic scabies
An oral product, Ivermectin, is available on a named person basis and has been used in combination with topical treatments for the treatment of hyperkeratotic (crusted, Norwegian or atypical) scabies that does not generally respond to topical treatment alone.
Patients with hyperkeratotic scabies may require 2 or 3 applications of topical treatment on consecutive days to ensure that enough penetrates the skin crusts to kill all mites.
14. Health and Social Care Settings e.g. Care Homes, Day Centres
Risk Assessment process:
It must be acknowledged that it will never be possible to completely eradicate the risk of scabies infection entering a care home setting or a day centre, so awareness of symptoms & early detection are key factors in limiting the impact of scabies infection within health & social care settings.
The purpose of the risk assessment process is to identify the potential source of scabies infection and then to take control measures that will minimise the impact of the infection within the setting.
If scabies infection is identified or suspected within a care home setting then the chance of possible infection for each resident and staff member should be assessed as ‘high’, ‘medium’ or ‘low’ risk, this will aide the appropriate follow-up and treatment of contacts.
High risk: are staff members who undertake intimate care of residents and who
move between residents, rooms or units. This will include both day & night staff. It will also include all symptomatic residents and staff members.
Medium risk: are staff and other personnel who have intermittent direct personal
contact with residents. It will also include asymptomatic residents who have their care provided by staff members categorised as ‘high risk’.
Low risk: those at lowest risk are staff members who have no direct or intimate
contact with affected residents e.g. gardeners, maintenance, catering & laundry staff. It also includes asymptomatic residents whose carers are not considered to be ‘high risk’ i.e. their direct personal care is provided by staff members who have not undertaken intimate care of symptomatic residents or who have not worked in the affected area(s) of the home.
All staff and residents identified as ‘high risk’ or ‘medium risk’ will require treatment even in the absence of symptoms. In many institutions this may involve all patients and staff, that provide direct resident care, being treated simultaneously (within a 24 hour period) in a co-ordinated way.
It is recommended that the management of care home facilities take responsibility for purchasing the scabicidal treatments for their staff. By doing this the home management can ensure that treatment is undertaken at the same time and will greatly reduce the risk of prolonged or re-infection.
There is no evidence to support the spread of scabies by fomites such as towels, bedding, soft furnishings or equipment. However, fomites may play a part in the dissemination of the more unusual form of scabies infection known as hyperkeratotic scabies (also known as crusted, Norwegian or atypical scabies).
Normal washing temperatures can be used and should be followed by thorough drying.
Care home staff do not need to stay off duty provided that they have observed the minimum contact time for their initial treatment.
Where staff have responsibility for applying the liquids/cream to residents, they should wear disposable non-sterile CE marked gloves to do so.
15. Principles of outbreak management and control
Definition of an outbreak:
The control of an outbreak of any infectious disease depends on early detection, investigation and appropriate control measures to prevent further spread.
For the purpose of a suspected outbreak of scabies, the following definitions can be applied:
• Two or more persons diagnosed with scabies by a clinician
• Two or more persons with an unexplained rash, diagnosed by a clinician as probable
Where there is a possible case of scabies infection specialist diagnosis should be undertaken by an appropriately trained person, i.e. dermatologist or dermatology nurse.
Single case of scabies infection:
Where an individual resident (single case) has a clinical diagnosis of scabies infection then they should be treated as soon as possible with an appropriate scabicidal treatment that has been prescribed by their GP (see section 11). They will require two full body treatments, seven days apart. Staff providing intimate care for this resident should be risk assessed as being ‘high risk’ and treated as appropriate i.e. two applications seven days apart for symptomatic staff & one application for asymptomatic staff. Cluster of cases / outbreak situation:
In the event of a cluster of cases/suspected outbreak of scabies, it is the responsibility of the owner, manager or nominated lead of the care facility to liaise with the local community infection control nurse (CICN) at the primary care trust (PCT) or local health protection unit (HPU) for support and advice. It may also be appropriate to liaise with the Care Quality Commission (CQC).
All GPs should be informed of the problem by the manager/officer in charge and should be requested to promptly see their patients to make a clinical diagnosis, to treat and to follow up as necessary.
Effective control requires early identification of index case(s) and adequate and simultaneous treatment (within a 24 hour period) of cases and close personal contacts to prevent further spread.
Treatment should be co-ordinated using the algorithm at Appendix 5 with all symptomatic care staff and residents in the affected area given two full body applications, seven days apart (see Appendix 1 & 2 for resident/staff recording sheet) Identified staff, residents and contacts who are asymptomatic only require one full body application (see Appendix 3 & 4 for resident/staff recording sheet).
If possible, have one principle pharmacy co-coordinating the supply of scabicidal treatments.
Family members of staff may require treatment if they have prolonged skin-to-skin contact and therefore should seek advice from their respective GPs.
Regular visitors to the home should also be advised about the scabies outbreak and given advice on the symptoms of scabies & where appropriate to seek treatment from their GP.
The management of the home should also post a notice in a public area of the home to inform visitors that an outbreak of infection is currently being experienced (Appendix 6). Management should consider, & discuss with their PCT CICN, the need to temporarily close to admissions / respite patients.
Care institutions that have recently had an admission or taken a transfer of a resident from an affected area (hospital ward or care home) should be informed so that an assessment of the patient can be made for possible infection risks.
For any further advice please contact the Community Infection Control Nurse at the Primary Care Trust or the local Health Protection Unit 16. References
Hawker, J., Begg, N., Blair, I. Reintjes, R. Weinberg, J. (2005) Communicable Disease Control Handbook. 2nd Edition, Blackwell Science.
DH (2006) Infection control guidance for care homes. DH Publications. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4136381
British National Formulary, September 2009, No.58, BMJ Publishing Group, London.
Insect Research and Development Ltd. (2004) Scabies. www.insectresearch.com Health Protection Agency Website www.hpa.org.uk CDC (2007) Scabies fact sheet
http://www.cdc.gov/Ncidod/dpd/parasites/scabies/factsht_scabies.htm
Appendix 1 Name of Care Home ………………………
Signs of scabies at 14 Signs of scabies at 21 days? If yes retreat, if days? If no, no further no, action, if yes retreat and Residents diagnosed with a scabies rash no further treatment* obtain specialist advice from CICN/HPA dermatologist* Treatment 1 Treatment 2 Circle Yes/No
*please note any residents who have signs of new infection at 14 or 21 days may require oral treatment this must be discussed with the GP or dermatologist (Photocopy more copies as needed)
Appendix 2 Name of Care Home ………………………
Signs of scabies at 14 Signs of scabies at 21 days? If yes retreat, if days? If no, no further Staff diagnosed with a scabies rash action, if yes retreat and no further treatment* obtain specialist advice from CICN/HPA dermatologist* Treatment 1 Treatment 2 Circle Yes/No * please note any staff who have signs of new infection at 14 or 21 days may require oral treatment this must be discussed with the GP or dermatologist. (Photocopy more copies as needed) Appendix 3 Name of Care Home ………………………
Signs of scabies infection at 7 days? Residents without a rash If yes retreat, and follow up as residents of Unit or Floor diagnosed with scabies (appendix 1). If no, no Treatment 1 further treatment (Photocopy more copies as needed)
S:\Infections and Diseases\Meetings\NW Policy group\Policies\Reviewed documents\Scabies%20in%20the%20Community.doc
Appendix 4 Name of Care Home ………………………
Signs of scabies infection at 7 days? Staff without a rash If yes retreat, and follow up as residents of Unit or Floor diagnosed with scabies (appendix 1). If no, no Treatment 1 further treatment (Photocopy more copies as needed)
S:\Infections and Diseases\Meetings\NW Policy group\Policies\Reviewed documents\Scabies%20in%20the%20Community.doc
Appendix 5
Reproduced by kind permission of the Medical Entomology Centre
Insect Research & Development Limited
S:\Infections and Diseases\Meetings\NW Policy group\Policies\Reviewed documents\Scabies%20in%20the%20Community.doc
APPENDIX 6
The home is currently experiencing an outbreak of scabies infection. We would like to assure all visitors and relatives that expert advice has been sought and all appropriate actions are being undertaken. If you would like to know more about scabies infection, an information leaflet is available from staff who are happy to discuss any concerns that you may have. Thank You
documents\Scabies%20in%20the%20Community.doc FINAL VERSION: 16/08/2010
Authorization for Medication Return form to school with Parent and Health Care Provider signatures Student Name ______________________________________________________ Date of Birth Parent’s Name Phone (home) Emergency Contact Name Phone (home)________________Cell___________________ When the district has received written orders from the student's physician and writt
Copyright SAFESPOT Deliverable D3.2.1 Dissemination Level (RE) Contract N. IST-4-026963-IP SAFESPOT INTEGRATED PROJECT - IST-4-026963-IP DELIVERABLE SP3 – SINTECH– Innovative Technologies Technical Scenarios Description for Positioning, Local Dynamic Maps and Vehicular Ad Hoc Networks Deliverable No. (use the number indicated on
 HEALTH PROTECTION AGENCY NORTH WEST
HEALTH PROTECTION AGENCY NORTH WEST 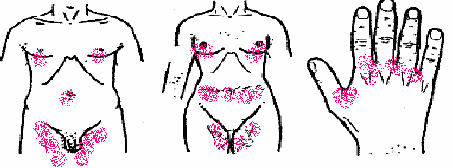 Recognition/Diagnosis
Recognition/Diagnosis