EVALUATION OF FAMILIES OF INFANTS WITH VERY LOW BIRTH WEIGHT IN HOME CARE 1 Anelize Helena Sassá2, Sonia Silva Marcon3
1 This study is part of the thesis - Nursing care delivery to infants with very low birth weight and families at home, presented
to the Graduate Nursing Program (PSE) at Universidade Estadual de Maringá (UEM), 2011.
2 M.Sc. in Nursing. Faculty Member, Nursing Department, Fundação Faculdade de Filosofia Ciências e Letras de Mandaguari.
Paraná, Brazil. E-mail: [email protected]
3 Ph.D. in Nursing Philosophy. Faculty, Nursing Department, UEM. Paraná, Brazil. E-mail: [email protected]ABSTRACT: Convergent care research which aimed to evaluate families of babies with very low birth weight, based on the Calgary
Family Assessment Model. The nine families included were attended for six months after the infant’s discharge from hospital. Data were
collected through home visits and analyzed based on the structural, functional and development categories proposed in the Calgary
Model. Conflicting subsystems were present only in one family and all families’ support network contained elements from other systems
than the family. The collaboration of parents, grandparents and older children in the household allowed the mothers to spend more
time taking care of the infants and contributed to a positive adaptation and family balance. Living with infants with very low birth
weight requires that families organize themselves and adapt to the home care, involving changes in the roles of each family member. DESCRIPTORS: Family. Infant, very low birth weigth. Child care. Nursing. AVALIAÇÃO DE FAMÍLIAS DE BEBÊS NASCIDOS COM MUITO BAIXO PESO DURANTE O CUIDADO DOMICILIAR RESUMO: Pesquisa convergente-assistencial cujo objetivo foi avaliar famílias de bebês nascidos com muito baixo peso baseando-se no
Modelo Calgary de Avaliação Familiar. Participaram nove famílias que foram assistidas durante seis meses após a alta hospitalar do
bebê. Os dados foram coletados por meio de visitas domiciliares e analisados com base nas categorias estrutural, de desenvolvimento
e funcional propostas pelo Modelo. Subsistemas conflituosos estiveram presentes apenas em uma família e todas apresentaram em
sua rede de apoio elementos oriundos de outros sistemas, que não o familiar. A colaboração dos pais, avós e filhos mais velhos nas
tarefas domésticas permitiu às mães dedicarem mais tempo aos bebês e favoreceu a adaptação positiva e o equilíbrio familiar. Conviver
com bebês nascidos com muito baixo peso exige que as famílias se organizem e se adaptem para o cuidado no domicílio, envolvendo
mudanças nos papéis de cada membro familiar. DESCRITORES: Família. Recém-nascido de muito baixo peso. Cuidado da criança. Enfermagem. EVALUACIÓN DE LAS FAMILIAS DE BEBÉS NACIDOS CON PESO MUY BAJO CUIDADO DEL HOGAR RESUMEN: Investigación convergente asistencial cuyo objectivo fue evaluar las familias de los bebés nacidos con muy bajo peso basado
en el Modelo Calgary de Evaluación de la Familia. Participaron nueve familias, que fueron atendidas durante seis meses después de la
alta hospitalaria del bebé. Los datos fueron colectados a través de visitas domiciliarias y se analizaron sobre la base de las categorías de
desarrollo, estructural y funcional propuesto por Modelo Calgary. Subsistemas en conflicto se presentaron sólo en una familia y todas
presentaron en su red de soporte elementos derivados de otros sistemas afuera los elementos familiares. La colaboración de los padres,
los abuelos y de niños más viejos en las tareas del hogar permitió a las madres dedicar más tiempo al cuidado de los bebés y favoreció
la adaptación positiva y el equilibrio de la familia. Convivir con bebés nacidos con muy bajo peso exige de las familias organización y
adaptación a los cuidados en el hogar, y implica en cambios en los papeles de cada miembro de la familia. DESCRIPTORES: Familia. Recién nacido de muy bajo peso. Cuidado del niño. Enfermería.
Text Context Nursing, Florianópolis, 2013 Abr-Jun; 22(2): 442-51.
Evaluation of families of infants with very low birth weight. INTRODUCTION
focusing on the needs that emerged in this context
Care represents a vital phenomenon in hu-
and stimulating coping mechanisms for each unit
man beings’ lives, based on human identity itself, and the child him/herself.9
marked by coexistence and interrelations,1 in a
relationship of exchange and sympathy.2 It is a the family permits the observation of interactions
way of being and being with the other that mainly between its members and the events that affect
refers to special issues in people’s lives, including the individual and collective functioning of each,8
the preservation and recovery of health, birth and and, thus, support for nursing care delivery in this
even death.1 As a form of interaction and personal context, the aim in this study was to assess families
involvement, care can be understood as solicitude, of infants with very low birth weight (VLBW),
dedication and concern for the other;2 and implies based on the Calgary Model.
caregivers’ knowledge, behaviors, skills and at-
titudes, influenced by their social, cultural and THEORETICAL FRAMEWORK
The family can be understood as the primary (CFAM) is a multistructural model that intends to
care unit as, through family experiences, values evaluate families and gain knowledge and skills
and beliefs are created and cultivated which for possible interventions needed. It involves the
contribute to the formation of its members, who concepts of system, cybernetics, communication
interact mutually, supporting each other and and change and consists of three main categories:
exchanging experiences, so as to search together structural, development and functional.
and add up efforts to surpass limits and solve
The structural category comprises the fam-
ily structure, that is, who is part of it, what is the
The birth of a child and his/her insertion in affective bond among its members and what is its
the family context require adaptations and changes context. The most used instruments to assess the
in the roles and tasks of each family member, who family structure are the genogram and ecomap.
attempt to respond to the infant’s demands for In graphical terms, the genogram represents the
affection and care and to organize the new family internal family structure and the ecomap is a dia-
gram, showing the family’s contact with the social
context and its affective bonds, representing the
ever, associated with very low birth weight family’s important connections with society.8
(VLBW<1500g), the infant needs hospitalization,
The developmental category is intended to
unexpectedly changing the family dynamics. The understand what moment in the lifecycle the fam-
prematurity events and the VLBW need to be ily has reached and, thus, to describe its trajectory.
elaborated, dealing with the child’s hospitaliza-
It values the predictable and unpredictable events
tion and possible complications and problems, that mark the family’s development cycle, so as
organizing the daily routine to accompany the to identify the events that create changes and de-
baby during hospitalization and preparing for mand the reorganization of family roles and rules.
The functional category, then, refers to how
Each family is unique and experiences this family members interact. Instrumental functioning
process in its own way. Therefore, it is important relates to daily activities, while expressive func-
to get to know the family, understand its behavior, tioning regards communication styles, problem
feelings and the meanings of this experience6 and, solving, roles, beliefs, rules and alliances.
based on knowledge about each premature infant’s
This model contributes to nurses’ work with
specific family contexts, attempt to promote care the family, based on a more reflexive perspective,
centered on their individual needs, acknowledging allowing its members to acknowledge their weak-
them as subjects who maintain relations with their nesses and value their potentials in order to better
Nurses involved in care delivery to these
children and their families are responsible for
minimizing the consequences of contact with METHODOLOGICAL TRAJECTORY
prematurity and VLBW, with a view to facilitat-
A descriptive and qualitative research was
ing changes and the regaining of family balance,8 carried out, using Convergent Care Research Text Context Nursing, Florianópolis, 2013 Abr-Jun; 22(2): 442-51.
(CCR) as a methodological framework.10 CCR those relatives who were at home during the meet-
is a recent method whose main characteristic is ing participated. In addition, information about
the intentional articulation between research and the researcher’s observation was used. As other
meetings happened, the instruments were comple-
The study subjects were members of nine mented when making registers in the field diary.
families living in Maringá-PR, in which Infants
with Very Low Birth Weight (IVLBW) were care and research processes, permits the use of
born between May and October 2010, who were different data collection and analysis methods.10
included in the city’s Surveillance Program for In this study, content analysis was used,11 charac-
terized by a technique that applies to the analysis
The SPIR is coordinated by the Municipal of written texts or any communication, with a
Health Secretary and exists since the year 2000. It view to understanding what lies behind each con-
is aimed at following infants with different risk tent manifested. The analytic process took place
factors, such as low birth weight and prematurity, through repeated readings of the field diaries,
every month during the first year of life. Therefore, which were allocated in the structural, develop-
the Epidemiological Surveillance Team visits ment or functional assessment categories proposed
maternity hospitals in the city daily to identify in the Calgary Model. Therefore, a table was used,
and include children at risk in the program. After which the researcher herself had elaborated, giv-
including the child, a reference form is forwarded ing rise to relevant interpretations and inferences
to the primary health care unit in the family’s about the family assessment.
coverage area for the purpose of accompaniment.
The research project received approval from
The families were located and included in the Permanent Ethics Committee for Research
the study based on the SPIR form, in compliance Involving Human Beings at Universidade Es-
with the criteria: a) infant’s birth weight <1500g tadual de Maringá (Opinion 309/2010). All ethi-
and b) living in Maringá-PR. In total, 43 individu-
cal premises required in National Health Council
als participated, including: 10 IVLBWs (one pair Resolution 196/96 were complied with. Thus,
of twins), nine mothers, eight fathers, 14 siblings, after explaining about the research objectives,
one grandmother and one uncle. Although all fam-
participation form and rights, the subjects who
ily members participated in the study indirectly, accepted to participate signed two copies of the
as members of the family unit, only the mothers informed consent form. To guarantee the families’
were present during all meetings, characterizing anonymity, participants were identified using fic-
them as central subjects and as the main research titious names, based on the feelings that marked
the care process for IVLBW during the six months
Data were collected between June 2010 and after hospital discharge.
August 2011, through Home Visits (HVs) that were
scheduled in advanced according the family’s care
needs, or with a minimal frequency of one monthly RESULTS AND DISCUSSION
HV during the first six months of accompaniment.
Next, the analysis of the data and discus-
The families received the first HV between the sion of the results will be presented according the
second and 21st day after hospital discharge. The categories proposed in the Calgary Model.
mean interval between discharge and the first HV
was eight days. On average, each family received Structural assessment
nine visits, ranging between six and 12 visits dur-
ing the six months after the IVLBW’s discharge.
During the HV’s, besides care, informal, semis-
nuclear families (except for the family Zeal), two
tructured interviews were held and participants of which had been reconstituted (Families Joy
observation was used, including records in a field and Strength) and one was a single-parent family
diary to permit further analysis and the achieve-
(Friendship Family). One was an expanded fam-
ily, as the couple and their children lived with the
To structure the genogram and ecomap, in-
maternal grandmother and uncle (Family Zeal).
formation was used about the family structure and
The fathers’ age ranged between 30 and 49
context, which the families themselves described years (mean age 38 years) and only one of them
in a specific interview whe, besides the mother, did not have a paid job (Hope family). Among
Text Context Nursing, Florianópolis, 2013 Abr-Jun; 22(2): 442-51.
Evaluation of families of infants with very low birth weight.
the mothers, ages ranged between 29 and 41 years maternity leave (Families Hope, Joy and Zeal). As
(mean 34 years); two did not have an external job for parity, three mothers were primipara (Families
before the pregnancy (Families Friendship and Union, Kindness and Friendship) and only three
Love), three decided to take a leave of absence couples had planned the pregnancy (Families
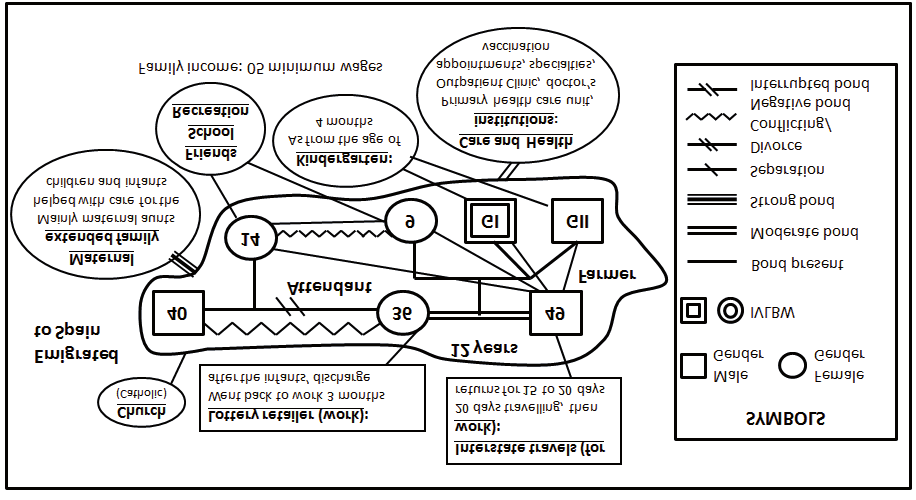
after the birth of the IVLBW (Families Union, Union, Friendship and Strength). Figure 1 graphi-
Kindness and Affection), one organized the work cally represents the family Joy, showing examples
environment to receive the infants (twins) (Family of the genogram and ecomap constructed during
Strength) and three returned to their job after their the evaluation. Figure 1 - Genogram and ecomap of the family Joy. Maringá-PR, June 2010 till January 2011
Twin pregnancies were present in two of which affected the infant in the family Love.
families (Joy and Strength). In the first, only one
The mean hospitalization time of the IVLBW
of the infants showed VLBW (1360g), due to an at the Neonatal Intensive Care Unit (NICU) was
Intrauterine Growth Restriction (IGR). In the 39 days, ranging between 13 and 109 days. The
Strength family, in which the multiple pregnancy mean total length of hospitalization was 60 days,
resulted from artificial insemination, both infants ranging between 22 and 120.
were born weighing less than 1500g, but with an
All mothers were able to take care of their
important difference (GI=655g and GII=1375g), infants during the hospitalization at the rooming-
due to abnormal implantation of the placenta and in unit after the discharge from the NICU. Only
the mother from the family Joy decided not to stay
All infants were born through caesarean at the rooming-in unit, dividing her time between
birth, and seven were male. The gestational age the second twin, who was already at home, and the
at birth ranged between 27 and 35 weeks (mean first twin, who was attended at the intermediary
29w3d) and weight between 655 and 1490g (mean care unit. This fact did not deprive her from tak-
1206g). Among the hospitalization diagnoses of ing part in care for the IVLBW as, during her stay
the IVLBW, the following stood out: respiratory at the hospital, she was encouraged to take care
distress syndrome (seven cases) early neonatal of her child. The family Strength negotiated with
infection (four), pneumonia (four), pneumothorax the hospital so that the mother could stay at the
(three), physiological jaundice (three), prematurity rooming-in unit with the two infants, although one
apnea (three), IGR (two), inguinal hernia (two), could already go home. This was possible as, due
necrotizing enterocolitis (one), persistent arterial to complications deriving from his birth condition,
canal), convulsive crisis (one), Down Syndrome the first twin was hospitalized much longer than
(one) and bronchogenic cyst (one), the latter three his sister. In addition, this family had sufficient Text Context Nursing, Florianópolis, 2013 Abr-Jun; 22(2): 442-51.
financial resources to hire accommodations in an hospitals, pharmacies), clubs, gym and the work
apartment instead of the nursing ward.
environment, thus constituting these families’
The subsystems identified in the internal social and support network.
structural assessment referred to relations between
For the family Friendship, the presence of
husband and wife, parents and children, grand-
the support network was fundamental do cope
mother and grandson, mother and infant, among with the separation and the mother’s need to take
others. Most of these served to maintain the fam-
care of the child and raise him alone. Although
ily unit and deliver care to the child. Conflicting the mother felt insecure and weakened, with the
subsystems were present in the family Hope only. help of friends, health services and church, she
The relationship between mother and adolescent was capable of getting organized to take care of
child was characterized by a hardly affective inter-
the IVLBW and restructuring as a family.
action, with turbulent dialogues and the mother’s
In the structural context evaluation, it was
lack of control over the adolescent’s behaviors. observed that social class and financial condition
The couple’s subsystem (father and mother), even did not influence the quality of care delivery to
before the pregnancy, was also disjointed, without the IVLBW at home. The mother’s need to go back
any expression of affection and complicity, which to work soon to help and provide for the family,
demonstrated that they stayed together for the the repeated dislocations to schedule specialized
mere sake of allowing both to continue following consultations in the public health system and the
the children’s growth and development.
fact that she needed support from relatives and
The situation was aggravated by the preg-
friends to take charge of child care and house-
nancy and birth of the daughter with VLBW. None work during her leaves demanded further efforts
of the members perceived the circular causality from those families with more limited financial
of their relations (attitudes of one interfering in resources (Families Hope, Joy, Friendship, Love
the other’s conduct, behavior and feelings), and and Affection).
they did not even notice how the way they acted
interfered in the other members’ posture inside Performance Assessment
the family context. As she needed but did not re-
ceive support from her husband, the woman saw
him as hardly interested in the family and, on the place at the same time, but the changes do not
opposite, the husband considered his wife as per-
necessarily happen equally in all family members.8
manently dissatisfied. The fact that the husband Concerning families of IVLBWs, it is obvious that
was unemployed also bothered the woman, who all of them had reached the stage of “families with
considered that he made little effort to help and small children”. This stage suggests changes and
provide for the family, while he believed he was tasks to adjust the marital system and make room
doing everything within his reach, taking on odd for the children; the union between the parents and
jobs to help and buy diapers and infant formula other family members to accomplish housework,
for the infant. In this process, the adaptive interac-
care for the infant and financial solutions; and the
tion among the members took a negative form as, realignment of relationships with the extended
after the change the birth of the IVLBW brought family to include the roles of the fathers, grand-
about, the established family balance revealed mothers and siblings.8
even greater distancing between husband and wife
Five families (Hope, Joy, Zeal, Strength
and between parents and children. The mother and Love) had simultaneously reached the stage of
completely took charge of care for the infant and “families with adolescent children”. The prevalent
made efforts to see to all needs: even during her task in this phase is to let the parent and child re-
maternity leave, she accepted days of cleaning to lationship allow the adolescent to enter and leave
increase the family income, arranged someone the family system, in search of new identities and
to stay with the infant while she was working, independence. In the families studied, however,
organized her time to keep the child’s medical all stages were articulated with the fact of having
follow-up up to date, and was also responsible a small child at home and this required particular
for all housework and care for the other children.
adaptations from each family member, including
As regards the external structure, all families the adolescents. Like some fathers, the older sib-
presented elements from other systems than the lings started to engage in housework to allow the
family, including friends, church, healthcare insti-
mothers to spend most of their time taking care of
tutions (primary health care units, medical offices, the infants. For the family Love, for example, the
Text Context Nursing, Florianópolis, 2013 Abr-Jun; 22(2): 442-51.
Evaluation of families of infants with very low birth weight.
change in its members’ routine and roles, associ-
herself from the former family conception (father,
ated with the IVLBW’s special needs, allowed the mother and children) and acknowledging herself
mother to abandon excessive zeal with the older in a new family composition, as a “mother without
children, delegating responsibilities for their acts a partner”. In addition, it was observed that some
and decisions, as well as greater demands related subsystems and existing bonds were strength-
to housework, which culminated in a relation of ened (with the maternal extended family, church
greater trust and commitment between mothers friends and community, from whom she received
emotional, material and financial support), while
In the family Hope, however, the adolescent others were undone or weakened, like the bond
son displayed weakened bonds with the other fam-
with the child’s father and his family, with whom
ily members and, although he sought psychologi-
she started to have a tense and hostile relationship
cal independence, the boy had to continue living while awaiting the divorce, accompanied by a
with the parents, even if in a conflicting manner, lack of demonstrations of affection and kindness
Two families (Joy and Strength) had reached
the late “second honeymoon” stage. This stage is Functional assessment
noteworthy because of the new family’s biased
organization, with new roles and relations among
As part of the functional assessment process,
the instrumental assessment revealed that the
change stage had already occurred and the fami-
mothers not only continued being responsible
ly’s stability had already been demonstrated. Only for housework, but also had to assume most care
the family Joy showed a conflicting relationship for the IVLBWs. Although all mothers had gone
between sisters, as the youngest, due to having through the experience of taking care of their chil-
the same degree of kinship as the twins, felt privi-
dren during the hospitalization, during the first
leged when compared to the older sister, who was days after discharge, taking care of the infant and
born from the mother’s earlier relationship. This taking charge of housework contributed to make
situation encouraged feelings of ownership and some of them feel exhausted, overloaded and
right on the small siblings, as well as on the fam-
insecure, mainly about seeing to their children’s
ily’s attention. The parents’ posture contributed needs, who demanded constant attention for
towards a positive adaptive interaction though, breastfeeding, maintenance of the weight gained,
as none of them treated the sons/stepdaughter basic hygienic care, sleep and rest, health monitor-
differently, and demonstrated this at all times, in ing and special consultations.
conversations, decision making and at times of
In view of this problem, during the first days
after discharge from hospital, some mothers felt
The family Friendship, in turn, displayed a the need for help from extended family members
different form. After eight years of union and vari-
(grandparents and aunts/uncles of the child) to
ous frustrated attempts to get pregnant, including help them take care of the IVLBWs, which made
the husband’s treatment, when he found out about them feel safer. This happened mainly in those
the pregnancy, he left home without giving further families in which the mother was a primigravida,
explanations to his wife, who started to live alone or also when the mother had to go back to work
while expecting the baby, anguished because she within few months after the discharge, as the early
did not understand what had happened. Even birth and VLBW obliged the mother to use part
when the pregnancy condition worsened, the of her maternity leave to accompany the infant’s
couple did not reconnect and, after the birth, the hospitalization.
father did not establish any affective and care
The support from other family members (fa-
bond with the child, offering only small amounts ther, child, grandparents) and their participation in
of money to the family. This implied the remain-
care and small tasks (Families Union, Strength and
ing family’s need to accomplish all tasks related Love) facilitated the family reorganization after the
to childcare and education. The mother assumed IVLBW arrived at home and resulted in a faster
tasks like: adjusting to the new marital status, play- adaptation and equilibrium when compared to
ing the role of care and financial provider with-
other families without positive interaction among
out her partner’s presence, seeking support and its members (Families Hope and Friendship).
financial restructuring/employment, detaching
The presence of significant people, includ-
Text Context Nursing, Florianópolis, 2013 Abr-Jun; 22(2): 442-51.
ing friends and other extended family members,
Religious belief and spirituality were present
although they did not directly participate in as a facilitator in family development and in the
care for the infants, was a positive factor in the infant’s welcoming at home. These represented
families and the infant’s adaptation process at help and hope to deal with the prematurity, as well
home. In the family Friendship, the mother fully as important instruments for the family evolution,
took charge of housework and care for the infant. the children’s education and the acceptance of and
For her, the presence of a friend to sleep at home coping with adversities.
during the first days after the discharge made
Problems were solved effectively in most
her feel supported, understood and less lonely, families. Although some situations caused diffi-
which strengthened her to cope with the delicate culties, resulting from the child’s birth condition,
situation she was going through. In addition, this such as the infant’s fragile appearance and size,
mother could count on the support and availabil-
the need for weekly medical appointments and
ity of friends and the community when she had the monitoring of breastfeeding and weight gain,
to be absent to solve issues like looking for a job the families demonstrated dynamic and effective
and forwarding the documents for the divorce. As problem-solving abilities, using the resources
stability was achieved in each period, however, available in each family and social context and
mother and child conquered more autonomy and the support received during nursing care at home.
organization in view of attention and care needs,
which permitted the gradual inclusion of leisure
and relaxation into daily activities, such as excur-
REFLECTING ON FAMILY INTERAC- TIONS AND HOME CARE FOR THE IN-
Some families’ better financial condition FANT WITH VERY LOW BIRTH WEIGHT
granted them more flexibility to get organized for
care at home, allowing the mothers to take a leave fective and care member in the family space and
of absence from work or have employees at their context. At the same time as the parents feel happy
disposal to help with housework (Families Union, and relieved after the infant’s discharge, they also
Kindness and Strength). For the family Affection, feel anxious and insecure12 about the new care
however, the couple jointly decided on the wom-
phase that is starting, distant from the hospital
an’s resignation from her job, weighing financial team. In the phase they are entering, adaptations
issues and the benefits the mother’s full-time stay and readjustments of the existing family bonds
could entail for the child. This process culminated and subsystems are needed, as well as of the roles
in the decision to resign, even if this implied a pe-
each family member assumed, with a view to fur-
riod of greater financial hardship for all members. thering attendance to the infant’s needs and his/
In the Strength family, then, as the mother did not her inclusion in the family context.
want to give up care for her children but had to
The infant’s arrival determines changes in
reassume her management function in the industry the family’s way of being, thinking and living, so
she owned, she adapted the work environment and that all members desire and get involved in care
prepared a place in her office for cradles, strollers for the child.13 When the pregnancy is not planned
and/or desired, however, the family can face the
The expressive assessment revealed that, in need for double coping, in which it will need to
those families in which effective communication accept the new family condition and get organized
existed among its members, that is, in which each to receive the new member. All this is aggravated
member understood and considered the other’s by the early interruption of pregnancy, the need
message, care delivery to the IVLBW took place for hospitalization in neonatal units and special
in a calm manner, including the exchange of tasks care demands when the child goes home.
and experiences. In the family Hope, however,
The entire family context influences the fam-
communication happened indirectly, due to the ily’s coping and the care form it adopts towards
cold relation between the couple and other family the child, and the anxiety the VLBW condition
members. Countless financial difficulties and the created can further compromise the family routine,
partner’s unemployment inhibit any feeling of enhancing limitations, weaknesses and conflicts
affection the women could have for her partner, and impairing the ability to solve problems and
whose messages were rejected and did not exert cope with adversities. In view of these families’
any influence on the family’s behavior.
vulnerability, it is important for health profes-
Text Context Nursing, Florianópolis, 2013 Abr-Jun; 22(2): 442-51.
Evaluation of families of infants with very low birth weight.
sionals, especially nurses, to be able to identify the care offered to the IVLBW at home, as the parent
weaknesses and potentials of the family relation-
without a partner starts to accumulate most tasks,
ship context the child was inserted in and, from which both parents would share in other family
that point onwards, to attempt to expand new configurations, in many cases accompanied by a
sources of support and the social network, in ac-
reduction of the resources available.8 This entails
an additional responsibility for the mother, who
It was verified that, initially, the families of IV-
makes more efforts to perform her tasks, like tak-
LBW were insecure about care for the infant and, as ing care of her own and her infant’s health (food,
they gained positive experiences during care, receiv-
medical and nursing appointments, vaccination,
ing support from other family members or from the medication purchase and administration, etc.),
social network, they felt safer and more confident to social control (financial resources, facing the com-
take care of organize the family development tasks.
munity after the divorce) and tension control in
Social support can be defined as a “system view of the vulnerability situation experienced. As
of interpersonal relations, with emphasis on the perceived, however, the father’s absence was com-
availability of help in situations of need”.15:55 The pensated for by the mother’s dedication or by other
presence of the support network is often character- factors, like the social support received.19 Thus,
ized as a protective component for mothers during when a change takes place in the family, after the
care delivery to the IVLBW at home as, feeling disorder (separation, premature and VLBW birth,
supported, they demonstrated greater security hospitalization, etc.), a change happens in search
to take charge of care for the child, according to a of a condition of balance, getting reorganized or
logic of autonomy and health promotion.16
rebalanced differently from the previous family
In addition, many families were able to count organization.8 This new family organization, at its
on their own members’ support, including the different levels, is perceived in several ways, and
reorganization of domestic and family activities, often goes beyond the home environment, reach-
so as to minimize the burden for the burden and ing the work environment and the social relations
to allow her to dedicate more time to care for the (adapting the workplace to receive the children,
infant. This type of family support benefits care avoiding travels and excursions, or adjusting these
for the child and grants security and tranquility routines to the child’s limitations and/or needs).
Another point highlighted is that, nowadays,
For some families, more complex adapta- a considerable amount of women have a paid job,
tions were needed, considering the stage of family partially or fully contributing to the family income.
development. This fact can be understood when As a result, mothers of small children have a triple
considering the family as a dynamic unit, which work journey, taking responsibility for their job,
therefore does not follow a single course. New housework and the newest task, which is care for
arrangements, with families based on free unions, the infant. For families with strengthened subsys-
single-parent families with a female or male tems, the division of housework and responsibili-
head, couples who get divorced and constitute ties for the children facilitates the adaptation to
new families, demonstrate families’ ability to get this period, so that the couple often remains more
transformed and create space for the establish-
cohesive as a result of its parental functions than
ment of different relationship forms.18 Although of its marital relationship, with a stronger bond in
the families in this study showed points of family the parental subsystem than among the partners.20
disorganization at first, like the conflict between
The social class and financial conditions did
sisters, little by little, these families got restruc-
not impede appropriate care delivery to the IV-
tured in their own manner and found mechanisms LBW, but demanded greater efforts from families
to solve the difficulties experienced. In addition, to with more limited resources. For these families,
the extent that they found solutions, these families the less favorable socioeconomic conditions influ-
started to live more harmoniously with the char-
enced their ability to organize their daily live and
acteristics the family constitution itself imposed.
respond to the challenges the arrival of the new
Single-parent families, like in the family baby at home imposed.8
Friendship, required intense adaptive resources
Belief and spirituality are part of human
due to aspects related to parental absence, which beings and, for the families of IVLBWs, these can
had occurred recently and without any causal represent the axis of balance and hope to face the
explanation. This family condition influences the difficulties the child’s birth condition imposed. To Text Context Nursing, Florianópolis, 2013 Abr-Jun; 22(2): 442-51.
the extent that the families are able to overcome
thought for nursing care. Rev Esc Enferm USP. 2009
challenges, they feel grateful for divine providence
and get strengthened in their faith. Another rel-
2. Backes DS, Sousa FGM, Mello ALSF, Erdmann AL,
evant point is that, in families with small or ado-
Nascimento KC, Lessmann JC. Care conceptions:
lescent children, spiritual values and principles are
an analysis of Ph.D. dissertations presented in a
accepted as educational guidelines, representing
nursing graduate program. Texto Contexto Enferm.
The family’s care is aimed at preserving the 3. Arruda DC, Marcon SS. The family in expansion:
life and health of each family member, especially
experiencing intercurrences during pregnancy and
childbirth of a very low weight premature baby.
the infant, so as to fully develop their potential,
Texto Contexto Enferm. 2007 Jan-Mar; 16(1):120-8.
in accordance with their own possibilities and
the conditions provided by the means they live 4. Bradalize DL, Zagonel IPS. A conceptual framework
for the care of the child’s family member with
in.21 Thus, solutions for the problems and difficul-
congenital heart disease, based on Roy’s theory.
ties that emerge in the course of this process are
Cogitare Enferm. 2006 Set-Dez; 11(3):264-70.
targeted and conquered, as the family is willing 5. Figueiredo MHJS, Martins MMFS. Family
to look for the resources available in its context,
assessment: from calgary family assessment model
whether through joint activities or isolated from
to the focus of nursing practice. Cien Cuid Saude.
the support network, so as to respond to all needs
6. Ribeiro NRR. The family facing the serious illness
of the child. In: Elsen I, Marcon SS, Silva MRS (Org).
FINAL CONSIDERATIONS
The life family and its interface with the health and
the illness. Maringá (PR): EDUEM; 2004. p.183-97.
The CFAM permits understanding families’ 7. Gaíva MAM, Ferriani MG. Prematurity: children
multiple dimensions and the use of the genogram
and family experienca. Acta Paul. Enferm. 2001
and ecomap provides a rapid image of family rela-
tions and a more comprehensive understanding 8. Wright LM, Leahey M. Enfermeiras e famílias: um
about the interaction between its members and
guia para avaliação e intervenção na família. 4ª ed.
Living with infants with very low birth 9. Vieira CS, Mello DF, Oliveira BRG. O seguimento
weight requires that families organize themselves
do prematuro e baixo peso ao nascer egresso da
and adapt to the home care, involving a series of
terapia intensiva neonatal na família: uma revisão de
changes in the functions and roles of each member
literatura. Online Braz J Nurs [online]. 2008 [acesso
in the family unit. The presence of the support
2011 Ago 12]; 7(3). Disponível em: http://www.
network mitigates coping with difficulties during
objnursing.uff.br/index.php/nursing/article/
this process and strengthens the family to see to
the child’s needs based on the context they live in.
10. Trentini M, Paim L. Pesquisa Convergente
Assistencial: um desenho que une o fazer e o pensar
na prática assistencial em Saúde-Enfermagem.
structures, relations and tasks sustain the adap-
tation period when the family starts to take care 11. Bardin L. Análise de conteúdo. Lisboa (PT): Edições
of the infant with very low birth weight at home,
further understanding and care solutions emerge 12. Rabelo MZS, Chaves EMC, Cardoso MVLML,
to support nursing care and actions, allowing pro-
Sherlock MSM. Feelings and expectations of mothers
fessionals to help family members to identify their
of preterm babies at discharge. Acta Paul. Enferm.
weaknesses and potentials, stimulating and advis-
ing them in the search for more effective forms of 13. Costa SAF, Ribeiro CA, Borba RIH, Balieiro MMFG.
care organization, with a view to promoting the
The family’s experience when interacting with the
healthy growth and development of the child and
premature newborn at home. Esc Anna Nery. 2009
14. Viera CS, Mello DF, Oliveira BRG, Furtado MCC.
REFERENCES
Social net and family social support in the following
of the preterm newborn and of low birth weight.
1. Silva IJ, Oliveira MFV, Silva SED, Polaro SHI,
Rev Eletr Enf [online]. 2010 [acesso 2010 Jun 20];
Radunz V, Santos EKA et al. Care, self-care and
12(1):11-9. Disponível em: http://www.fen.ufg.br/
caring for yourself: a paradigmatic understanding
Text Context Nursing, Florianópolis, 2013 Abr-Jun; 22(2): 442-51.
Evaluation of families of infants with very low birth weight.
15. Guimarães EC, Melo ECP. Characteristics of social
conceptions about paternity, parenthood and gender
support associated with prematurity in a population
relations in female heads of households. Psicol Clin.
of mothers of low income. Esc Anna Nery. 2011 Jan-
19. Marin A, Piccnini CA. One-parent families: single-
16. Simioni AS, Geib LTC. Perception of the mothers
mother in the literature. Psico. 2009 Out-Dez;
concerning the received social support in home care
to the premature children. Rev Bras Enferm. 2008 20. Fleck AC, Wagner A. The woman as the principal
responsaible for the economic home support. Psicol
17. Soares DC. Living with the extreme premature and
his family in the hospital and home context. Rev Eletr 21. Delgado JA. The family living deeply health-illness
Enf [online]. 2008 [acesso 2010 Jun 20];10(3):864-5.
situations: a knowledge in construction. In: Elsen
Disponível em: http://www.fen.ufg.br/revista/
I, Marcon SS, Silva, MRS, organizadores. The life
family and its interface with the health and the
18. Perucchi J, Beirão AM. New family arrangements:
illness. Maringá (PR): EDUEM; 2004. p.385-94.
Text Context Nursing, Florianópolis, 2013 Abr-Jun; 22(2): 442-51.
5.3 Atemschutzmasken Ob Atemschutzmasken vor Infektionen allgemein wirksam schützen, ist nicht eindeutig bewiesen, da keine unumstrittenen Wirksamkeitstests vorliegen, die mit lebenden oder abgetöteten Keimen durchgeführt worden wären. Es gibt jedoch – aus der Erfahrung mit SARS – Hinweise dafür, dass die Übertragung von Viren durch Atemschutzmasken eingeschränkt werden kann. Bei
PORT OF LOS ANGELES SCHOOL BOAT TOUR PROGRAM FREQUENTLY ASKED QUESTIONS Who is my Port of Los Angeles School Boat Tour contact? Trisha Malahni, Direct number: (310) 732-3960 Public Relations Division main line: (310) 732-3508 Email: [email protected] How can I find information about the School Boat Tour Program? Schools interested in participating in the Port of Los An
 Evaluation of families of infants with very low birth weight.
Evaluation of families of infants with very low birth weight.