Evaluation of insulin-like growth factor-I in postmenopausal women with breast cancer treated with raloxifene
Benedito Borges da Silva, Cleicilene Gomes Pires, Edílson Carvalho Sousa-Junior,
Alesse Ribeiro dos Santos, and Pedro Vitor Lopes-Costa
Department of Gynecology, Federal University of Piauí, Teresina, Piauí, BrazilCorresponding author and requests for reprints:
Benedito Borges da Silva, M.D, Ph.D.
Avenida Elias João Tajra, 1260, Apt. 600, Bairro Jockey Club
Running title: IGF-I and breast cancer Abstract Background: The objective of this study was to evaluate serum IGF-I levels in
postmenopausal women with breast cancer treated primarily with raloxifene. Methods:
Twenty-two postmenopausal patients with operable, stage I or II, estrogen receptor-
positive carcinomas participated in this study. Following confirmation of diagnosis, the
patients received 60 mg of raloxifene for 28 days prior to definitive surgery. Blood
samples were collected for evaluation of serum IGF-I levels prior to initiating
medication and following a 28-day treatment course. Student’s t-test for paired samples
was used in the statistical analysis. Significance was established at p<0.05. Results:
Mean serum IGF-I levels pre- and post-raloxifene treatment were 143.7±9.7 ng/ml and
94.8±7.6 ng/ml, respectively. This reduction in serum IGF-I levels following treatment
with raloxifene was statistically significant (p<0.001). Conclusions:
significantly reduced serum IGF-I levels in postmenopausal women with breast cancer. Key words: breast; cancer; IGF-I; raloxifene; SERMs. Background
Insulin-like growth factor-I (IGF-I) is produced principally in the liver upon
stimulation by GH and plays an important role in promoting normal and neoplastic cell
proliferation [1-8]. Insulin-like growth factors I and II are almost exclusively bound to
IGF binding proteins (IGFBPs), less than 1% circulating freely [7]. There are six types
of IGFBP; however, more than 90% of all circulating IGF-I is bound to IGF binding
protein-3 (IGFBP-3) [7,9,10]. IGFBP-3 inhibits the action of IGF-I at cell level by
competitively binding IGF-I and thereby preventing it from binding to the IGF-I
The IGF system is currently recognized as a risk factor for the principal types of
epithelial cancer [11,12]. Studies have shown an association of increased serum levels
of IGF-I and decreased levels of IGFBP-3 with an increased risk of breast cancer in
premenopausal women [13,14], suggesting that these patients may benefit from
measures able to reduce serum IGF-I levels and increase IGFBP-3 levels. Nevertheless,
a few studies have shown that some therapeutic strategies have succeeded in reducing
serum IGF-I levels but without altering IGFBP-3 levels [2,7]. Steroidal and non-
steroidal antiestrogens have been previously shown to inhibit the growth of estrogen
receptor (ER)-positive cells, not only by acting as competitors of hormone agonists on
nuclear receptors, but also by preventing the mitogenic action of the growth factor in the
Significantly reduced serum IGF-I levels have also been reported in
postmenopausal women with breast cancer treated primarily with tamoxifen [1,3].
However, tamoxifen exerts an estrogen-agonistic effect on the endometrium and when
used for long periods of time increases the risk of endometrial carcinoma 3-4-fold in
postmenopausal women [16], a fact that has triggered a search for alternative SERMS
for the chemoprevention and treatment of breast cancer [17]. Raloxifene is a second-
generation SERM that was initially approved by the US Food and Drug Administration
for the prevention and treatment of osteoporosis; however, it was found to exert an
antiestrogenic effect on the breast without stimulating the endometrium [18,19]. This
fact was confirmed in the recently published Study of Tamoxifen and Raloxifene
(STAR) trial, which showed that raloxifene is as effective as tamoxifen in reducing the
risk of invasive breast cancer, as well as reducing the risk of endometrial carcinoma
To the best of our knowledge, only one study published in the literature has
evaluated the effects of raloxifene, administered for a period of 14 days prior to surgery,
on serum IGF-I levels as a primary treatment for breast cancer in postmenopausal
women [2]. It is possible that women may benefit from the use of raloxifene over a
longer period of time, both in chemoprevention and in the treatment of breast cancer.
Therefore, in view of the paucity of reports in the literature on the primary effects of
raloxifene on serum IGF-I levels in postmenopausal women with breast cancer, we
decided to carry out the present study in which medication was administered for 28 days
Patients and Methods Patients: The protocol of this study received the approval of the Institutional
Review Board of the Federal University of Piauí. All volunteers gave their signed,
informed consent prior to initiation of the study. Twenty-two postmenopausal women
in amenorrhea for at least two years, who had sought medical care at the Mastology
Department of the Federal University of Piauí and who had been diagnosed with
operable, estrogen-receptor-positive, invasive ductal carcinoma for which they had
received no prior treatment, were enrolled to this study. Following hematoxylin-eosin
staining and confirmation of the diagnosis of invasive ductal carcinoma, the paraffin
blocks containing the samples underwent histochemical analysis to evaluate estrogen
Tumors with nuclear staining measured semiquantitatively as high
(>10% immunoreactive cells) were considered positive. Patients with endocrinopathies,
those in use of hormonal medication or any other medication that could interfere with
serum IGF-I levels were excluded from the study. Tumors ranged from 2 to 5 cm in
size, stages I or II. Patients were aged 47 to 87 years (mean 63 years). Treatment: The patients received 60 mg of raloxifene/day for a period of 28
days prior to definitive surgery, starting at the time of confirmation of the diagnosis
Sample collections: For the analysis of serum IGF-I levels, two fasting blood
samples were taken, one at baseline, i.e. prior to the initiation of raloxifene therapy, and
the second after a 28-day course of the treatment.
centrifugation and aliquots were stored at -20oC until assayed. All tests were carried out
by a professional who was blinded with respect to patient identification. Assay method:
For the analysis of the serum concentrations of insulin-like
growth factor-I, the automated immunoassay analyzer, DPC Immulite 2000 (DPC Inc.,
Los Angeles, USA) was used, and methodology consisted of a solid-phase enzyme-
labeled chemiluminescent immunometric assay. Analytic sensitivity was 20 ng/ml and
the reference values varied according to age. Statistical methods: Comparison of the means of serum IGF-I levels measured
prior to and after 28 days of raloxifene use was carried out using Student’s t-test for
paired samples. Statistical significance was established at p<0.05.
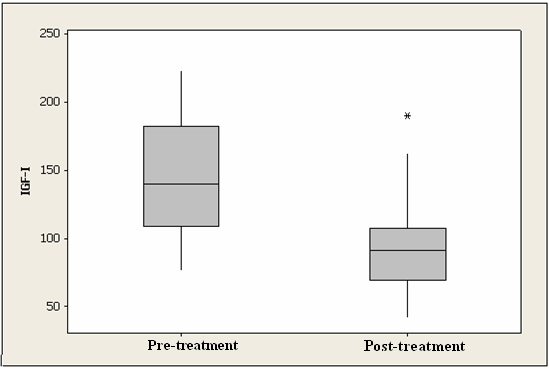
Mean pretreatment serum IGF-I level was 143.7±9.7 ng/ml, whereas mean post-
treatment serum IGF-I level was 94.8 ± 7.6 ng/ml (Table 1).
statistically significant (p<0.001). The box-plot clearly shows a reduction in the median
serum levels of IGF-I evaluated 28 days after the use of raloxifene in postmenopausal
patients with breast cancer (Figure 1). Discussion
Insulin-like growth factors are potent mitogens for the proliferation of breast
cancer cells [1]. Insulin-like growth factor-I is a potent mitogen for breast cancer cell
lines and it is now accepted that elevated IGF-I levels are a risk factor for breast cancer
in the premenopause [3]. Therefore, women at risk of breast cancer or patients with
neoplasia may benefit either preventively or therapeutically from strategies to reduce
SERMs have been shown to reduce both circulating and
microenvironmental levels of IGF-I, thereby suppressing IGF-induced growth of both
ER-positive and ER-negative breast cancer cells [1]. Nevertheless, the adverse effects
of tamoxifen, principally stimulation of the endometrium, have evoked interest in
studying other SERMS that may have a lesser negative effect or no negative effect on
the endometrium and a similar or greater efficacy in chemoprevention or in the
treatment of breast carcinoma [16,17].
In the present study, raloxifene, at a dose of 60 mg/day for 28 days, significantly
reduced serum IGF-I levels in postmenopausal women with estrogen receptor-positive
breast carcinoma. The schedule of 28 days of use of the medication by postmenopausal
women prior to surgery was chosen with the intention of administering the drug for a
longer period of time; however without delaying definitive surgery, 28 days being the
mean time in our institute between the first consultation and surgery. In addition, the
dose of 60 mg of raloxifene was chosen because it is the most commonly used dose for
the prevention and treatment of osteoporosis and in clinical trials in the
chemoprevention of breast cancer [19]. Serum levels of IGBP-3 were not evaluated;
however some studies have shown no changes following the administration of
raloxifene, except a decrease in the IGF-I/IGFBP-3 molar ratio following raloxifene
treatment [2]. Our study was not placebo-controlled, and therefore subjects were not
randomized to a treatment regimen. A placebo-controlled study would have had distinct
design advantages over the study described here; however, controversies on the ethical
implications of such trials have been the subject of recent collaborative reports [3,21].
Our findings of a reduction in serum IGF-I levels in postmenopausal women
with breast cancer following treatment with raloxifene are in agreement with data
published by other investigators [2]. The study of serum IGF-I levels only in women
with estrogen receptor-positive tumors does not appear to be an issue since SERMs
reduce serum IGF-I levels both in women with estrogen receptor-positive and negative
tumors [1,22]. Apart from their main action via estrogen receptors, SERMs possess
numerous other plausible mechanisms for controlling tumor growth, such as binding to
protein kinase C and inhibiting angiogenesis [22,23]. An experimental study has shown
angiogenesis inhibition in an estrogen receptor-negative animal model, suggesting that
the antiangiogenic effects of SERMs are partially due to mechanisms that do not depend
on estrogen receptors [24]. In addition, reports from other experimental studies have
suggested the possibility that the action of antiestrogens does not occur only via
estrogen receptors but also by direct inhibition of growth factors [22], which may
explain the response of some estrogen receptor-negative breast tumors to SERMs.
Interest in the role of the insulin-like growth factor (IGF) axis in carcinogenesis
has grown following the finding of elevated serum levels of insulin-like growth factor-I
in association with the principal forms of epithelial cancer [9,12]. In addition, IGF-I is
a systemic hormone with potent anti-apoptotic and mitogenic properties that may
influence the proliferative behavior of breast cells [14]. Raloxifene has been shown to
be effective in inhibiting cell proliferation both in normal and in neoplastic breast tissue
According to one recent report, the drug significantly reduced Ki-67 antigen
expression in the breast tissue of premenopausal women [17]. Finally, the reduction in
serum IGF-I levels by raloxifene in postmenopausal women with breast cancer supports
the need to conduct further clinical trials on adjuvant therapy and chemoprevention with
References
1. Winston R, Kao PC, Kiang DT: Regulation of insulin-like growth factors by antiestrogen. Breast Cancer Res Treat 1994; 31: 107-115.
2. Torrisi R, Baglietto L, Johansson H, Veronesi G, Bonanni B, Guerrieri-Gonzaga
A, Ballardini B, Decensi A: Effect of raloxifene on IGF-I and IGFBP-3 in postmenopausal women with breast cancer. Br J Cancer 2001; 85: 1838-
3. Campbell MJ, Woodside JV, Secker-Walker J, Titcomb A, Leathem AJ: IGF status is altered by tamoxifen in patients with breast cancer. Mol Pathol
2001; 54: 307-310.
4. Eng-Wong J, Hursting SD, Venzon D, Perkins SN, Zujewski JA: Effect of raloxifene on insulin-like growth factor-I, insulin-like growth factor binding protein-3, and leptin in premenopausal women at high risk for developing breast cancer. Cancer Epidemiol Biomarkers Prev 2003; 12: 1468-1473.
5. Gronbaek H, Tanos V, Meirow D, Peretz T, Raz I, Flyvbjerg A: Effects of tamoxifen on insulin-like growth factors, IGF binding proteins and IGFBP- 3 proteolysis in breast cancer patients. Anticancer Res 2003; 23: 2815-2820.
6. Laban C, Bustin SA, Jenkins PJ: The GH-IGF-I axis and breast cancer.
Trends Endocrinol Metab 2003; 14: 28-34.
7. Furstenberger G, Senn E, Morant R, Bolliger B, Senn HJ: Serum levels of IGF- 1 and IGFBP-3 during adjuvant chemotherapy for primary breast cancer. Breast 2006; 15: 64-68. Premenopausal levels of circulating insulin-like growth factor I and the risk of postmenopausal breast cancer. Int J Cancer 2006; 118: 1279-1284.
9. Grimberg A, Cohen P: Role of insulin-like growth factors and their binding proteins in growth control and carcinogenesis. J Cell Physiol 2000; 183: 1-9.
10. Duschek EJ, Gooren LJ, Netelenbos C: Comparison of effects of the rise in serum testosterone by raloxifene and oral testosterone on serum insulin-like growth factor-1 and insulin-like growth factor binding protein-3. Maturitas
2005; 51: 286-293.
11. Mantzoros CS, Tzonou A, Signorello LB, Stampfer M, Trichopoulos D, Adami
HO: Insulin-like growth factor 1 in relation to prostate cancer and benign prostatic hyperplasia. Br J Cancer 1997; 76: 1115-1118.
12. Yu H, Spitz MR, Mistry J, Gu J, Hong WK, Wu X: Plasma levels of insulin- like growth factor-I and lung cancer risk: a case-control analysis. J Natl Cancer Inst 1999; 91: 151-156.
13. Hankinson SE, Willett WC, Colditz GA, Hunter DJ, Michaud DS, Deroo B,
Rosner B, Speizer FE, Pollak M: Circulating concentrations of insulin-like growth factor-I and risk of breast cancer. Lancet 1998; 351: 1393-1396.
14. Toniolo P, Bruning PF, Akhmedkhanov A, Bronfer JM, Koenig KL, Lukanova
A, Shore RE, Zeleniuch-Jacquotte A: Serum insulin-like growth factor-I and breast cancer. Int J Cancer 2000; 88: 828-832.
15. Vignon F, Bouton MM, Rochefort H: Antiestrogens inhibit the mitogenic effect of growth factors on breast cancer cells in the total absence of estrogens. Biochem Biophys Res Commun 1987; 146: 1502-1508.
16. Fisher B, Constantino JP, Wickerham DL, Redmon CK, Kavanah M, Cronin
WM, Vogel V, Robidoux A, Dimitrov N, Atkins J, Daly M, Wieand s, Tan-Chiu
E, Ford L, Wolmark N: Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst 1998; 90: 1371-1388.
17. da Silva BB, Lopes IM, Gebrim LH: Effects of raloxifene on normal breast tissue from premenopausal women. Breast Cancer Res Treat 2006; 95: 99-
18. Delmas PD, Bjarnason NH, Mitlak BH, Ravoux AC, Shah AS, Huster WJ,
Draper M, Christiansen C: Effects of raloxifene on bone mineral density, cholesterol concentrations, endometrium postmenopausal women. N Engl J Med 1997; 337: 1641-1647.
19. Cummings SR, Eckert S, Krueger KA, Grady D, Powels TJ, Cauley JA, Norton
L, Nickelsen T, Bjarnason NH, Morrow M, Lippman ME, Black D, Glusman JE,
Costa A, Jordan VC: The effect of raloxifene on risk of breast cancer in postmenopausal women: results from the MORE randomized trial. Multiple Outcomes of Raloxifene Evaluation. JAMA 1999; 281: 2189-2197.
20. Vogel VG, Constantino JP, Wickerham DL, Cronin WM, Cecchini RS, Atkins
JN, Bevers TB, Fehrenbacher L, Pajon Jr, Wade JL 3rd, Rabidoux A, Margolese
RG, James J, Lippman SM, Runowicz CD, Ganz PA, Reis SE, McCaskill-
Stevens W, Ford LG, Jordan VC, Wolmark N:
Effects of tamoxifen vs raloxifene on the risk of developing invasive breast cancer and other disease outcomes: the NSABP Study of Tamoxifen and Raloxifene (STAR) P-2 trial. JAMA 2006; 295: 2727-2741.
21. Fisher B, Powles TJ, Pritchard KJ: Tamoxifen for the prevention of breast cancer. Eur J Cancer 2000; 36: 142-150.
22. Gagliardi A, Collins DC: Inhibition of angiogenesis by antiestrogens. Cancer Res 1993; 53: 533-535.
23. da Silva BB, da Silva Junior RG, Borges US, da Silveira Filho MA, Pimentel IC,
Gebrim LH, Simões Mde J, Baracat EC: Quantification of angiogenesis induced in rabbit cornea by breast carcinoma of women treated with tamoxifen. J Surg Oncol 2005; 90: 77-80.
24. Blackwell KL, Haroon ZA, Shan S, Saito W, Broadwater G, Greenberg CS,
Dewhirst MW: Tamoxifen inhibits angiogenesis in estrogen receptor- negative animal models. Clin Cancer Res 2000;6:43-59. Figure 1 Boxplot of serum IGF-I levels measured prior to and following 28 days of
raloxifene treatment in post-menopausal women with breast cancer. Additional files provided with this submission:
Group 1: Carcinogenic to Humans (108) ( 16 January 2009 ) Agents and Group of Agents 4-Aminobiphenyl [92-67-1] (Vol. 1, Suppl. 7, Vol. 99; in preparation) Aristolochic acid (Vol. 82, Vol. 100A; in preparation) (NB: Overall evaluation upgraded from 2A to 1 based on mechanistic and other relevant data) Arsenic [7440-38-2] and arsenic compounds (Vol. 23, Suppl. 7; 1987) (NB: This evaluation applies
The Management of Spasticity; The Evaluation and Treatment of An Interdisciplinary Approach Spasticity in Adults with ND/ID • Decrease spasticity • Infection (including urinary-tract) • Improve functional ability and independence • Constipation • Decrease pain associated with spasticity • Reflux • Prevent or decrease incidence of contractures • D
 Additional files provided with this submission:
Additional files provided with this submission: