A Case Study of South Africa’s PMTCT Policy Before and After the Treatment Action Campaign Social Movement1
Grace Tang2 Abstract In this paper, I investigate the history of preventing mother to child transmission (PMTCT) policy within the broader framework of South Africa’s approach to the HIV/AIDS epidemic. Then I look at the leadership that prevented or encouraged the improvement of PMTCT policy including former president Thabo Mbeki, former health minister Manto Tshabalala-Msimang, and social activist Zackie Achmat. I also explore other factors that may have contributed to the changes in PMTCT policy such as the government’s stance on intervention and the activism of lobby groups. In summarizing these factors, I investigate a possible explanation for the changes in the PMTCT policy and the implications for future policy.
1 Paper presented at the Comparative Responses to AIDS in Africa Conference, March 10, 2010
2 Fourth year International Development Studies undergraduate student, [email protected]Introduction
Vertical transmission of the human immunodeficiency virus (HIV) occurs when
mothers with HIV infect their child during pregnancy, during the delivery or post-partum
via breast-feeding. An intervention program is necessary in order to prevent infants from
contracting HIV and “without access to anti-retrovirals, about a third of vertically
infected young children die during the first 12 months of life, 50% by 2 years and 60% by
3 years" (Richter, 72). Prevention of mother-to-child-transmission (PMTCT) involves
the primary prevention of HIV to young women, antenatal care in the context of HIV
pregnant mothers, safe labor and delivery, and carefully planned post-natal care. While
most interventions focus on preventing transmission during pregnancy, the risks of
infecting an infant post-partum are still high, so attention must be paid to feeding
practices and adherence to self-administered drugs. High income countries have virtually
eliminated the threat of transmission, but sadly this is not the case in many developing
countries. Within sub-Saharan Africa, some countries are more successful and arduous
in their campaigns against PMTCT than others. Botswana, for example, has at least 95%
of mothers living with HIV receiving ARVs to reduce the risk of transmission in the 2008
national PMTCT policy (Universal Access, 101). Leaps and bounds have been made in
the battle against mother to child transmission recently, however historically speaking
South Africa’s government has interfered with access to ARVs for mothers, neglecting to
treat infected infants and to prevent the virus from being passed on. South Africa
currently only has governmental aid or coverage for less than 67% of infected mothers
living within its borders (National Antenatal Survey 2008). South Africa’s PMTCT
policy has been a subject of a larger struggle concerning the country’s delivery of anti-
retrovirals (ARVs) to people who are living with HIV. In this paper, I investigate the
history of the PMTCT policy within the broader framework of South Africa’s approach
to the crippling HIV/AIDS epidemic. I will further look into the specific leadership that
is preventing or encouraging the improvement of PMTCT policy. Specifically, I delve
into the policies of former president Thabo Mbeki, former health minister Manto
Tshabalala-Msimang, and social activist Zackie Achmat. The denialist stance that Mbek
took during his presidency impeded almost all HIV/AIDS related health progression and
prevented any foundation of a very necessary intervention program for preventing
infection of infants. Tshabalala-Msimang’s distrust of giving ARVs to pregnant women
only caused further transmission and stalled the formation of a national program which
prompted social activists to accuse the government of denying South African citizens the
right to health care. Achmat and the Treatment Action Campaign (TAC) pursued a court
case that would jump-start the use of ARVs on a national scale and governmental aid for
underprivileged mothers. After giving the political background of the case, I will also
explore other factors that have contributed to the PMTCT policy as it is known today,
such as the government’s stance on AIDS intervention and the power of lobby groups to
incite change. In summarizing these factors, I conclude with an explanation that
inneffective government leadership and the leanings towards dissident and denialist
ideals stalled the roll out of a national PMTCT policy. With the constant and tireless
efforts from TAC demanding explanations for the delays, bringing the issue to South
Africa's High Court, and filing and winning a constitutional claim against the government
for neglecting equality in access to health services were HIV pregnant women finally
able to have public access to life saving nevirapine.
Overview of 2000-2002 PMTCT Policy
Before the pilot program was introduced in South Africa, AZT or zidovudine was
already available in the Western Cape starting in 1999. Because the ANC was not in
control of the Western Cape during that time, the provincial government started programs
which ensured that the preventative medication was given to HIV infected pregnant
women. AZT had to be taken daily from 36 weeks of pregnancy which made successful
litigation of the drug for MTCT use more difficult than nevirapine. In 2000, a committee
of the Health Minister and the nine Provincial Members of the Executive Council (MEC)
for Health decided to first test nevirapine in two pilot test sites for every province in both
rural and urban areas. The Protocol for Providing A Comprehensive Package of Care for The Prevention ofMother to Child Transmission of HIV (PMTCT) in South Africa was
drafted in 2001 and provided an overview of how the government would initiate and
execute the pilot program. The protocol noted after the 13th International Conference on
HIV/AIDS in July 2000, there was enough scientific evidence confirming the efficacy of
ARVs in reducing the transmission of HIV from mother to child that it should be
implemented within the region immediately. But the operational challenges of actually
introducing an ARV regimen needed to be assessed in both rural and urban settings.
PMTCT not only included the ARV intervention of single dose nevirapine (SdNVP) and
Co-trimoxazole, but also voluntary counseling and testing (VCT), HIV testing, revised
obstetric practices and infant feeding practices. The protocol claimed these services
require ''extensive capacity building, infrastructure development, improved management
and community mobilization efforts" (Protocol 2001). The specific objectives
concentrated on the feasibility and acceptability on providing voluntary counseling and
testing services, medicine, and the monitoring and evaluation of patients living with HIV
or aids. The objectives of the pilot program wanted to test the capabilities of the current
health system on including more services geared toward prevention that would change
the priorities and services of antenatal care in the public health sector. The protocol
implemented only two sites for each nine provinces, totaling to only 18 test sites in urban
and rural settings. An estimation of 3,000 to 5,000 deliveries per year was expected at
each site, which included hospitals and hospitals and feeder clinics. All pregnant women
at the sites received basic antenatal care. They were offered, though not required,
information on the availability of PMTCT. If a woman enrolled she was provided with
counseling and testing. Women who tested positive were invited to join the program
giving them access to nevirapine and micronutrient supplements. They were also
counseled on appropriate infant feeding choices in context of preventing vertical
The limited coverage of the pilot program was decided because government
officials were skeptical of the drug efficacy and to prevent women and children from
other places from obtaining the drug until the two-year program established the safety of
SdNVP. The interim findings from the Health Systems Trust concluded “there are no
good reasons for delaying a phased expansion of PMTCT services in all provinces”
(McCoy). Since the dosages of nevirapine were limited to these test sites, other doctors
in public health could not administer the drug, limiting the number of pregnant women
who could actually receive treatment. The report indicated while PMTCT services
should be used to bolster the public health system, nevirapine and appropriate counseling
and information should be provided immediately to pregnant women who know their
HIV status (McCoy). The battle for public and free access to ARVs in South Africa
started with gaining treatment for HIV positive mothers.
Government Response and The Denialist Factor
Many who prevented the implementation of better access to ARVs for pregnant
women included former President Thabo Mbeki and his denialist and dissident leanings.
Another important leader who hindered the progression of care Health Minister Manto
Tshabalala-Msimang and her distrust of ARVs, which impeded and encapsulated the
government’s approach to HIV/AIDS. Mbeki’s public declaration of seeing no link
between HIV and AIDS led many in the global and scientific community to protest.
While Mbeki never outright stated his position on PMTCT, his silence lead South
Africa’s government to inaction on delivering life-saving ARVs that impeded the
progress of effectively combating HIV/AIDS. His doubts on the effectiveness and
toxicity of AZT also affected the leadership in the health department of fighting against
HIV/AIDS. His statements in 1999 criticizing the toxicity found in AZT brought forth
many dissident researchers who aligned with him in declaring a Western model of
intervention would not work in a sub-Sahara African setting. The group of AIDS
dissidends believed that ARVs destroyed the immune system instead of helping to restore
it. Mbeki’s alignment with the dissenters of HIV/AIDS meant that he did not believe
HIV caused AIDS, that immune deficiency was only possible from one virus (Rijn, 531).
His instead thought poverty was the cause of the AIDS epidemic and the reason why
babies were not being vaccinated. Mbeki and his government's response is in reaction to
the seemingly "racist representation of AIDS as a 'black disease' associated with sexual
promiscuity and the inability of Africans to control their sexual appetites." (Robins, 660)
This defensive stance of the government meant that access to ARVs was nearly
impossible because dissenters thought connecting HIV to AIDS meant creating a market
for ARVs, thereby prompting the 'medicalization of poverty.' In 2000, his government
denied an offer by Boehringer Ingelheim, a manufacturer of nevirapine, for a free five-
year supply of the much needed medicine called Viramune (Heywod, 285). The
infections of newborns could not be mitigated until that defense was challenged enough
to allow for a pilot program to be established in 2001.
The former president's position and the various AIDS myths, stigmas and shames
contributed to defensive responses and denial amongst members of his government. No
other government official was more outspoken and critical on the provision of anti-
retrovirals to pregnant women than his former health minister. Former Health Minister
Manto aligned with Mbeki politically as she also was in opposition to using AZT for
preventing MTCT. Her stance on the provision of nevirapine was that more research was
needed to prove that it was not toxic to pregnant women and children. She raised
concerns about the toxicity of nevirapine during a speech made to Parliament in April
2000 (Heywood, 284). Manto has influenced the testing of nevirapine because the
Medicines Control Council was a twenty four member committee appointed by her to
approve the use of nevirapine for stopping MTCT. The MCC has delayed the approval of
using nevirapine in MTCT for 16 months as claimed by two doctors (Gordin). Her
department’s drafted policy introducing SdNVP included a two-year research period,
which would determine the safety of the drug and viability of establishing a national
The Treatment Action Campaign
The Treatment Action Campaign and its most recognized leader, Zackie Achmat,
were responsible for challenging the government in their claims about the dangers of
ARVs for HIV infected mothers. Their efforts to request important documents detailing
the delays of rollling out the pilot program also revealed the political stalling done within
Manto's health department. TAC was established in 1998 to advocate for increased
access to treatment, care and support services for people living with HIV and to
campaign for reducing new HIV infections (TAC). The intial victories won by TAC
were by challenging pharmecutical companies to lowering the prices of essential
medicines (Heywood Law, 16). After Manto publically alligned with Mbeki with regards
to the safety of AZT and delaying the distribution of nevirapine to HIV infected mothers,
TAC had to face its own government in the court room. The lobbying and pressuring of
the government to provide AIDS treatment meant that clashes in ideologies and
prejudices held by the South African governmental departments were inevitable.
The basis of TAC’s strategy was concurrent with the biomedical and social
mobilization paradigm which advocated for more declarative and clear national political
leadership, mobilization of resources to combat the epidemic, introduction of publicly
funded-exposure prophylaxis for rape survivors and, above all, the use of ARVs to
prevent mother-to-child transmission (Heywood). TAC's partner organizations included
Doctors Without Borders (MSF), Haroon Saloojee, a representative of pediatricians and
other health care workers, and other grassroots organizations. The two-year pilot
program was deemed an obstruction to providing full public coverage of nevirapine to all
HIV infected mothers and interfered with doctors' ethical responsibility to treat their
Saloojee was the representative of Save Our Babies, a group of health
professionals who pressed for the implementation of an effective program to reduce
MTCT. At least 150 health professionals expressed support for the goals of the group.
This group of pediatricians in 2000 organized a petition campaign in support for a MTCT
reduction program. Their voices and concerns were ignored or brushed aside by the
Ministry of Health (Court Case). Cati Vawda was the head of the Children's Rights
Center (CRC) in Durban which acted on behalf of children born or will be born in the
public health sector to HIV positive mothers. The CRC wanted to enforce the
constitutional rights of children, that no child was deprived of his or her right of access to
health services, and ensure the government took responsibility in preventing or reducing
MTCT (Court Case). The three groups had similar interests in demanding access to
antiretrovirals for full public use and reasons for the government's delay in establishing a
The Case for Antiretroviral Access
Movement for the court case against the government began in 2001 when the pilot
program was delayed by the health minister in giving access to SdNVP in the 18 pilot
sites. A letter from TAC's attorney demanding legally valid and ethical reasons why
nevirapine has not been made accessable as of July 2001 was sent to the health minister
Manto and the nine provincial MECs. Only Manto responded to the letter by stating
concern for the provision of the medicine but ultimately listing barriers such as the
inadequate health infrastructure that legitimizes the delay of the rollout (Heywood, 291).
TAC however, found faults in the response from Manto who admitted the ethical issue of
the policy was limiting public sector doctors from providing nevirapine to pregnant
women who already know of their HIV status. On August 21st, 2001, TAC and
associated organizations with a coalition of pedeatricians represented by Saloojee and the
CRC in Durban filed a constitutional claim against health minister Manto and the nine
MEC for Health in all provinces. A series of affidavits claim against the government that
limiting access of SdNVP to only pilot sites denies other patients at other sites the right to
'the undoubted benefits of Nevirapine' (Court Case). With the MCC's approval of the
drug, doctors other than those in pilot sites, should have the discretion to give the drug to
their patients. The evidence brought by TAC charged the government's conduct in
limiting the drug and failure over an extended period of time to implement an all
encompassing program for PMTCT was in violation of the Bill of Rights and 'contrary to
the values and priciples prescribed for public adminsitration' in South Africa's
The government responded in arguing again the dangers of nevirapine by citing a
study of long term use for treatment of HIV. It also accused doctors dispensing
nevirapine in non-pilot sites of being irresponsible. The decision of the case was decided
in favor of TAC after two days in December 14, 2001 by Judge Chris Botha. He ordered
the governemnt to develop a fully capable and effective national program to reduce
MTCT by the next year. Manto decided to appeal the decision, citing that the decision by
the judiciary crossed constitutional boundaries and interfered with the executive branch's
role in deciding matters for the country. The appeal was revoked in 2002 (Heywood
299). A new operational plan for treating and caring for those infected with HIV/AIDS
Expansion of the PMTCT Program
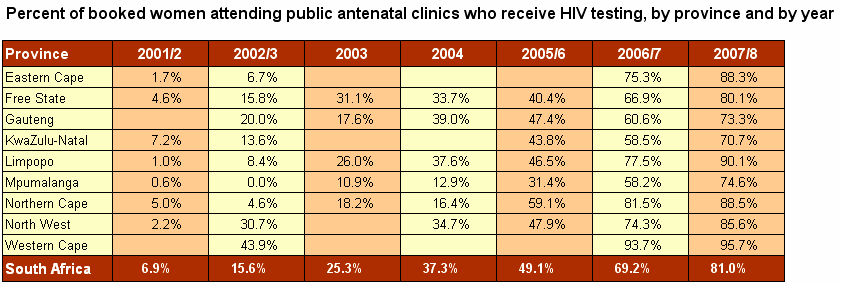
The Operational Plan for Comprehensive HIV and AIDS Care, Management and
Treatment for South Africa was released in November 19, 2003. It included an
expansion of the provision of SdNVP, extension of coverage to all HIV pregnant mothers
and their children and expansion of related services such as Voluntary Counseling and
Testing (VCT). HIV testing by women attending public antenatal clinnics has expanded
in uptake in all provinces (Johnson, 1).
This indicated the expansion of services related to PMTCT in the public sector and the
importance of testing would only reveal the status of HIV in pregnant women. This first
step of determing the HIV status of a mother is part of the sequential steps in order to
successfully prevent transmission of the HIV virus. Losses occured in between the steps
and not all participating women will receive the necessary medicine and post-partum care
such as correct infant feeding practices (Barometer 05/06, 44). In 2005, only half or
51.7% of tested mothers accessed nevirapine (55). In the years 2006 to 2007, about 65%
of tested mothers accessed nevirapine and the following year the percentage increase to
Conclusion
In summarizing these factors, I conclude that inneffective government leadership
and the leanings towards dissident and denialist ideals led to deny AZT as a possible
treatment for PMTCT. Mbeki's stance affected his government in the stalled the roll out
of a national PMTCT policy. The conduct of affairs by health minister Manto and the
Health department delayed the approval of nevirapine, a life saving drug which would
reduce the rate of HIV transmission to babies if administered under the guidance of a
health professional. TAC with its partner groups were constantly and tirelessly
demanding explanations for the delays, bringing the issue to South Africa's High Court,
and filing and winning a constitutional claim against the government. The case addressed
the neglect of equality in access to health services and HIV pregnant women were finally
able to have public access to life saving nevirapine. An appeal by the government was
denied in 2002 and a national PMTCT program was finally implemented in 2003 as part
of the national plan to address HIV/AIDS. The uptake of HIV testing and nevirapine in
all provinces improved gradually through the years since the program was implemented.
References
District Health Barometer 2005/2006. Health Systems Trust, 2006.
<http://www.hst.org.za/uploads/files/secA4.pdf>
District Health Barometer 2007/2008. Health Systems Trust, 2009.
<http://www.hst.org.za/uploads/files/dhb0708_sec4.pdf>
Gordin, Jeremy. 'MCC Held Up Release of Free AIDS Drug'. Cape Argus April 7,
2001. <http://www.iol.co.za/index.php?set_id=1&click_id=13&art_id=ct2001040719100624D620386>
Heywood, Mark. Preventing Mother-to-Child HIV Transmission in South Africa:
Background, Strategies and Outcomes of the Treatment Action Campaign Case Against the Minister of Health. South African Journal of Human Rights, 2003.
Johnson, Leigh. Access to Prevention of Mother to Child Transmission (PMTCT)
programmes: HIV Testing. Center for Actuarial Research, University of Cape Town, September 2009.
L. Richter et al. HIV/AIDS in South Africa 25 Years On, ed. P. Rohleder et al.
Springer Science+Business Media, 2009.
McCoy et al. Interim Findings on the National PMTCT Pilot Sites: Lessons and
Recommendations, Health Systems Trust, 2001. <http://www.hst.org.za/uploads/files/PMTCT_Interim.pdf>
MTCT Court Case. The Treatment Action Campaign vs the Health Minister and 9
MECs of Health, 2001. <http://www.tac.org.za/documents/MTCTCourtCase/ConCourtMOHVsTAC.txt>
Protocol for Providing a Comprehensive Package of Care For the Prevention of
Mother to Child Transmission of HIV (PMTCT) in South Africa, Version 5, 23 May 2001 <http://pmtct.org.za/docs/MTCTprotocol_v5.zip>
Rijn, Kiran van. The Politics of Uncertainty: The AIDS Debate, Thabo Mbeki and
the South African Government Response, Social History of Medicine, Vol. 19, No. 3, pp 521-538
Robins, Steven. 'Long Live Zackie, Long Live': AIDS Activism, Science and
Citizenship after Apartheid. Journal of Southern African Studies, Vol. 30, No. 3 September 2004.
World Health Organization. Towards Universal Access: Scaling up priority
HIV/AIDS interventions in the Health Sector, Progress Report 2009. <http://www.who.int/hiv/pub/tuapr_2009_en.pdf>
2-SPEED CORDLESS SCREWDRIVER _______________________________________________________________ 144 AFB 2,6 18,0 Volt / 2,6 Ah Technical specification Battery 1,5 – 13 mm Set includes Quick Action Chuck Ø 13 mm, Second battery pack, quick charger CSL 30 LI with cable depot, PH 2 screwdriver bit, Belt hook with integrated bit holder,
Ballybrown Equine Clinic, Ballybrown, Clarina, Co. Limerick, Ireland. Tel: +353 (0)61 353296 Fax: +353 (0)61 353352 Email: [email protected] Web: horsevet.ie EXPECTANT MARE Assuring the Health and Well-Being of the Pregnant Mare We often think of pregnancy as a delicate and fragile condition. When it comes to horses, this perception is perhaps due to the mare’s relatively poor reprodu
 299). A new operational plan for treating and caring for those infected with HIV/AIDS
Expansion of the PMTCT Program
299). A new operational plan for treating and caring for those infected with HIV/AIDS
Expansion of the PMTCT Program