O R I G I N A L C O N T R I B U T I O N
Continuous Versus Intermittent Nebulizationof Salbutamol in Acute Severe Asthma:
Lamia Besbes-Ouanes, MD* See editorial, p. 236. Semir Nouira, MD* Souhail Elatrous, MD‡ Study objective: This study was conducted to compare the Jalel Knani, MD*
clinical and spirometric effects of continuous and intermittent
Mohamed Boussarsar, MD* October 29, 1999. Revisions received
nebulization of salbutamol in acute severe asthma. Fekri Abroug, MD* February 17, 2000, andApril 3, 2000. Accepted forMethods: Forty-two consecutive patients presenting to the
emergency department for acute severe asthma (peak expira-
Address for reprints: Fekri Abroug,
tory flow [PEF] mean±SD, 24%±12% predicted) were prospec-
tively randomly assigned to receive 27.5 mg of salbutamol by
Bourguiba, Monastir 5000, Tunisia;216 3 460672, fax 216 3 460678;
either continuous or intermittent nebulization over a 6-hour
period. The continuous nebulization group received 15 mg of
salbutamol during the first hour and 12.5 mg over the next 5
hours. The intermittent nebulization group received 5 mg of
salbutamol every 20 minutes during the first hour and 2.5 mg
47/1/109169 doi:10.1067/mem.2000.109169
hourly over the next 5 hours. All participants received oxygenand intravenous hydrocortisone. Clinical and spirometricassessment was performed at baseline, 40 minutes, 60 min-utes, and at 3 and 6 hours after the start of the nebulization. Secondary endpoints were the respective rates of hospitaliza-tion and treatment failure. Results: A significant clinical and spirometric improvement was observed in both groups over baseline as soon as the 40th minute and was sustained thereafter (absolute PEF increase at the sixth hour 30%±18% and 32%±22% in the continuous and intermittent nebulization groups, respectively; P<.01 over base- line). PEF and the clinical score evolved similarly in both groups. There was no difference between the groups regarding the fail- ure rate of the initial bronchodilator treatment to terminate the asthma attack (3 [14%] in the continuous nebulization group and 2 [9.5%] in the intermittent nebulization group, absolute difference 4.5% [95% confidence interval –14% to 23%]). Eight (38%) patients and 9 (43%) patients from the continuous and intermittent nebulization groups, respectively, required hospital-
A N N A L S O F E M E R G E N C Y M E D I C I N E
S E P T E M B E R 2 0 0 0 C O N T I N U O U S V E R S U S I N T E R M I T T E N T N E B U L I Z A T I O N O F S A L B U T A M O L
ization according to predefined criteria (absolute difference
we designed this prospective, randomized, double-blind
4.8% [95% confidence interval –24% to 34%]).
study to test the hypothesis that an equal total dose ofsalbutamol nebulized continuously induces a greater
Conclusion: We did not observe an appreciable difference
bronchodilator effect and clinical improvement than
between continuous and intermittent nebulization of salbutamol
intermittent nebulization in acute severe asthma.
in acute severe asthma. The decision to use one of these nebu-lization methods should be based on logistical considerations.
[Besbes-Ouanes L, Nouira S, Elatrous S, Knani J, Boussarsar M,
All consecutive patients who presented to the emergency
Abroug F. Continuous versus intermittent nebulization of
department of our hospital, a tertiary teaching hospital,
salbutamol in acute severe asthma: a randomized, controlled
with acute exacerbation of asthma between March 1996
trial. Ann Emerg Med. September 2000;36:198-203.]
and June 1997 were screened. The following criteria wererequired for inclusion in the study: a measured peak expi-
ratory flow (PEF) of less than 50% predicted in associationwith 2 of the following clinical criteria of severity: heart rate
There is general agreement that nebulization of β -ago-
120 beats/min or greater, respiratory rate greater than or
nists is the mainstay of therapy in patients with acute
equal to 30 breaths/min, pulsus paradoxus greater than or
asthma,1,2 and inhalation represents the route of choice.3-6
equal to 15 mm Hg, accessory muscles contraction, SaO2
Bronchodilator inhalation allows the deposition of high
less than 92% on room air, and hypercapnia (>42 mm Hg).
doses of β -agonists directly to the bronchial receptors,
Arterial blood gas values were determined in all patients.
producing maximal bronchodilator effects with minimal
Exclusion criteria included a history of chronic cough, car-
systemic absorption and side effects. There is a consen-
diac or hepatic disease, or pregnancy. Patients were not
sus that frequent intermittent nebulizations (3 in the first
excluded when they had used β -agonists drugs delivered
hour) are appropriate,1,2,6-9 but continuous nebuliza-
by metered-dose inhaler before ED arrival. Patients were
tion is also proposed.1,2 Frequent administration of
allocated by means of random table to receive salbutamol
bronchodilators is thought to dilate the proximal
either by continuous or intermittent nebulization. After
bronchial tree, thereby allowing further distal deposition
opening of the sealed allocation envelopes, mixtures for
of subsequent bronchodilator treatments, which pro-
nebulization were prepared by an uninvolved ED staff
duces sustained bronchodilation and prevents bron-
member. The study physician was blinded to the solution
chospastic rebounds.10-13 All these benefits also might be
used and to the nebulization modality.
obtained with continuous nebulization of bronchodila-
All patients received a total dose of 27.5 mg of salbuta-
tors.13-18 Recent studies comparing intermittent and
mol (Ventolin for nebulization; GlaxoWellcome) over the
continuous nebulization of β -agonists suggested that
6-hour study period. Aerosol was administered by a
the latter might carry some advantages.14,15 However,
pneumatic nebulizer (mini-nebulizer; Peters; 40-115510;
these studies focused on pulmonary function change and
Bobigny, France) with a face mask driven by an oxygen
did not assess clinically relevant endpoints such as the
flow rate of 6 L/min. A bench test showed that a 5-mL
improvement of the clinical condition and the rate of
solution was delivered within 12 to 13 minutes. Patients
hospitalization or relapse. Moreover, beneficial effects
received 15 mg of salbutamol during the first hour and
were not found on an intention-to-treat basis and were
2.5 mg hourly thereafter. The reservoir of the pneumatic
apparent only when a retrospective post hoc analysis was
nebulizer was connected to a standard infusion pump by
performed on the subset of the patients exhibiting the
an 18-gauge needle. Syringes filled with 7.5 mL and 50
most severe bronchial obstruction.14,15 In addition, in
mL of saline solution (intermittent nebulization group) or
one study the regimen of intermittent nebulization did
salbutamol solution (continuous nebulization group)
not conform to that currently recommended for frequent
were successively delivered to the reservoir over the first
hour and over the next 5 hours, respectively. In addition,
Finding a better way to administer β -agonists might
the content of vials containing either saline solution (in
be of utmost importance because severe bronchoconstric-
the continuous nebulization group) or salbutamol (in the
tion and acute severe asthma has been well identified as
intermittent nebulization group) was added to the reser-
the leading cause of mortality in asthma.19 Accordingly,
voir every 20 minutes during the first hour, then hourly
S E P T E M B E R 2 0 0 0
A N N A L S O F E M E R G E N C Y M E D I C I N E
C O N T I N U O U S V E R S U S I N T E R M I T T E N T N E B U L I Z A T I O N O F S A L B U T A M O L
for the remaining 5-hour study period. Hence, each patient
Data are presented as mean±SD. Data were analyzed on
received a nebulization of 5 mL every 20 minutes the first
an intention-to-treat basis. Baseline data of the 2 groups
were compared using Mann-Whitney U test for non-nor-
In addition to nebulized salbutamol, all patients
mally distributed continuous variables. Changes in PEF
received oxygen delivered at a flow rate of 6 L/min and
rates and clinical severity scores were evaluated using
intravenous hydrocortisone hemisuccinate, 200 mg
repeated-measures analysis of variance with the time by
group as within-subject factor. Sample size calculations
Clinical evaluations and PEF (best of 3 measurements)
(β=.2 and 2-tailed α=.05) showed a study population of
were performed at baseline and after 40 minutes, 1 hour,
19 in each group would have an 80% power to detect a
3 hours, and 6 hours from the start of nebulization.
13% difference in PEF (assuming SD of 14%)15,20 and a
Clinical severity was measured by a scoring system that
2-point difference in clinical severity score (assuming SD
assessed 5 components (dyspnea, wheezing, accessory
muscles contraction, respiratory rate, and pulsus para-
The study protocol was approved by the local ethics
doxus), each rated on a score of 0 to 3 with a maximum
committee of our hospital, and informed consent was
score of 15 reflecting a severe attack.5 Patients had con-
obtained from each participating patient.
tinuous cardiac monitoring throughout the study periodand ECGs were obtained at the sixth hour. Arterial blood
gas values and serum potassium levels were measured atinclusion in the study and at the sixth hour.
During the study period, 102 consecutive patients pre-
In case of clinical deterioration during the study and
sented to the ED with acute asthma, and 42 fulfilled the
when the initial treatment protocol failed to terminate the
inclusion criteria and were randomly assigned to study
asthma attack, patients were admitted to the ICU andadditional treatment was given. Treatment usually con-sisted of nebulized ipratropium bromide and intravenous
aminophylline. At the end of the sixth hour, patients were
Baseline characteristics of study patients.
discharged from the ED when the following criteria werepresent: SaO greater than 92% on room air, no persistent
Continuous Intermittent
use of accessory respiratory muscles, pulsus paradoxus
Nebulization Nebulization
less than 12 mm Hg, PaCO less than 45 mm Hg, and pH
Characteristic
greater than 7.35 with a PEF value more than 60% pre-dicted.7 Patients who did not meet these criteria were
Primary outcome measures were changes in spiromet-
ric values and clinical scores. Spirometric improvement
Previous medication, No. (%)*
was assessed according to the magnitude and time course
of PEF change. Clinical improvement was assessed by a
change in the clinical severity score. In developing this
score, a reduction by 3 points reflected significant im-
provement in the asthma severity. Therefore, we consid-
ered the time needed to achieve a reduction by 3 points in
the clinical severity score, as well as the proportions of
Interval between attack onset and ED arrival (h)
patients in each group whose score was reduced by 3
points at the first evaluation time, to be clinically rele-
vant. Patients whose PEF or clinical severity score did not
improve during the first hour of the study were compared.
Secondary outcome measures were failure to improve rate
(with ICU admissions) and hospitalization rate.
The frequency of untoward β -agonist effects (heart
rate change, hypokalemia, and ECG changes) were also
*Some patients were receiving more than one medication.
A N N A L S O F E M E R G E N C Y M E D I C I N E
S E P T E M B E R 2 0 0 0 C O N T I N U O U S V E R S U S I N T E R M I T T E N T N E B U L I Z A T I O N O F S A L B U T A M O L
treatment. Demographic and clinical characteristics of
needed to reduce the clinical severity score by at least 3
the study patients are shown in the Table. Mean PEF was
points was not statistically different between both groups
24%±12% predicted. Hypoxemia was present in all
(114±9.3 minutes versus 102±9.4 minutes, respectively).
patients with a mean PaO /FIO ratio of 198±55 mm Hg,
All but 5 patients were successfully treated in the ED.
whereas hypercapnia was present in 35% of patients.
Three (14%) patients in the continuous nebulization
Twenty-one patients in each group were randomly
group and 2 (9.5%) patients in the intermittent nebuliza-
assigned to receive either continuous nebulization or
tion group did not improve and required supplemental
intermittent nebulization. Each group had identical
treatment (absolute difference 4.5%; 95% CI –14% to
demographic and clinical characteristics (Table).
23%). All these patients were hospitalized in the ICU and
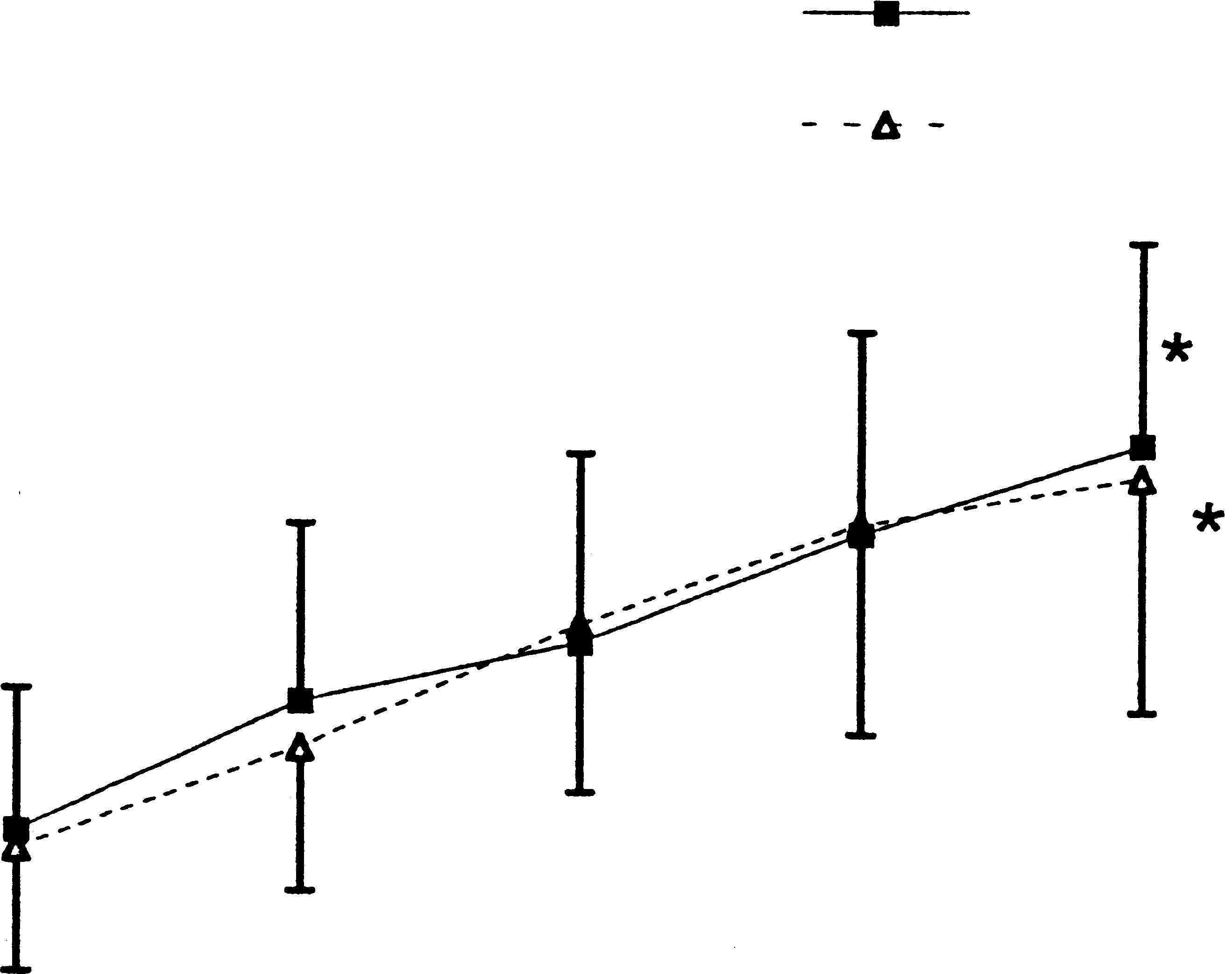
Both nebulization modalities improved PEF and clini-
received additional medications as needed. Mechanical
cal severity score compared with the baseline value. The
ventilation was required in only one patient from the
absolute PEF increase at the 6-hour evaluation time was
intermittent nebulization group. There were no deaths in
30%±18% and 32±%22% in the continuous and inter-
the study population. There was no statistical difference
mittent nebulization groups, respectively (P<.01 over
in the hospitalization rate between the study groups; 8
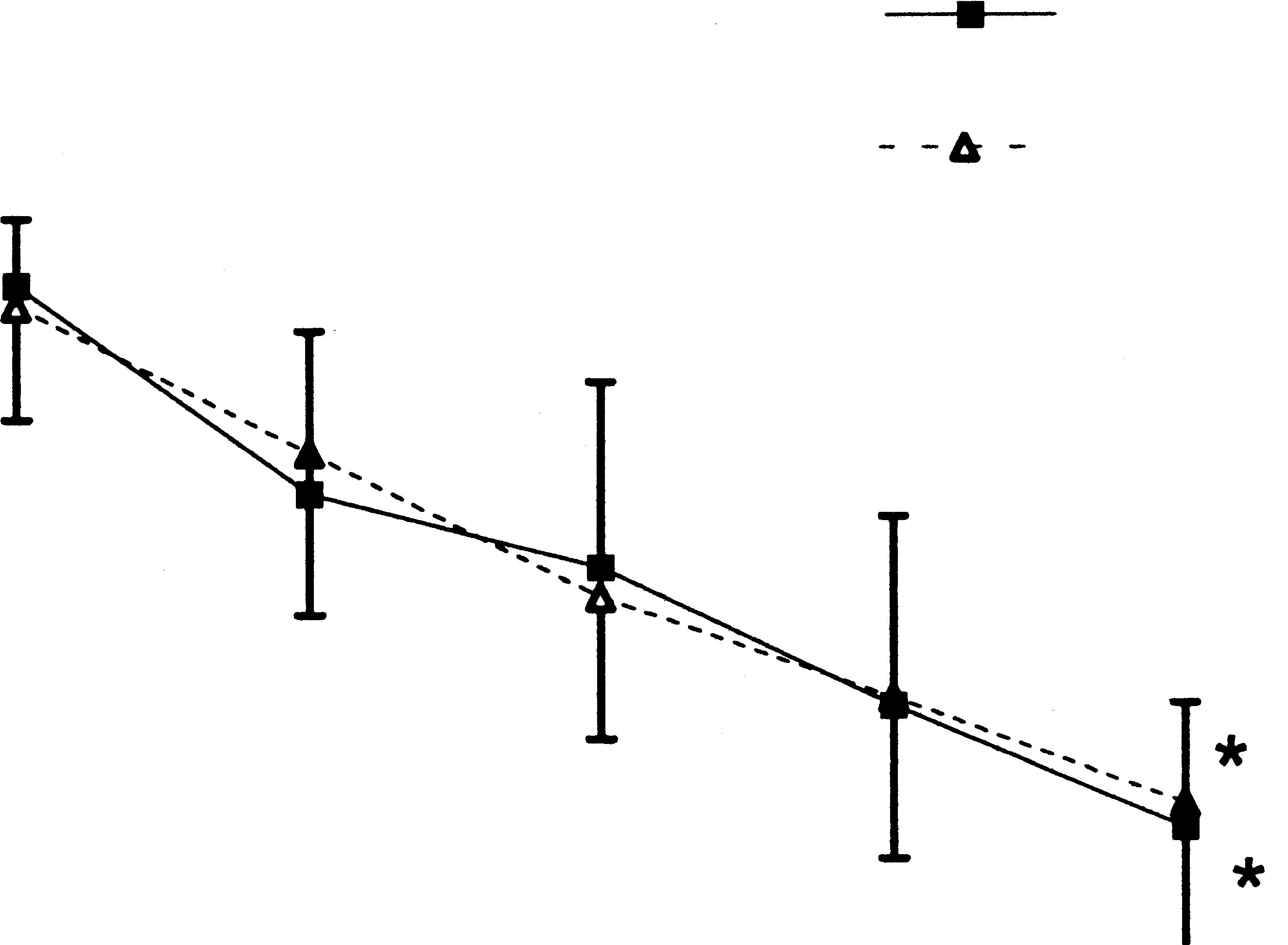
baseline) (Figure 1). The decrease in clinical severity
(38%) patients and 9 (43%) patients in the continuous
scores at the 6-hour evaluation time was 6.3±3.1 and
nebulization and intermittent nebulization groups,
6.1±2.9 in the continuous and intermittent nebulization
respectively, were hospitalized according to the prestated
groups, respectively (P<.01 over baseline) (Figure 2).
criteria (absolute difference 4.8%; 95% CI –24% to 34%).
Neither the magnitude nor the time course of PEF and
No major untoward effects related to salbutamol nebu-
clinical severity score improvement were statistically dif-
lization were recorded in the present study. In particular,
ferent between the study groups. Similar proportions of
the serum potassium concentration decreased by the
patients achieved a reduction by 3 points in the clinical
same magnitude in both groups (–0.44 and –0.40 mmol/L,
severity score by the 40th minute: 38% and 33% in the
respectively) and was slightly reduced at the end of the
continuous nebulization and the intermittent nebuliza-
study period (3.4±0.4 mmol/L and 3.6±0.4 mmol/L in the
tion groups, respectively (absolute difference 5%; 95%
continuous and intermittent nebulization groups, respec-
confidence interval [CI] –22% to 32%). The time interval
tively). The heart rate was also decreased by 20 and 18beats/min, respectively. No other ECG changes wereobserved in any of the study patients. Figure 1. Percent predicted PEF for continuous (solid line) and intermit-tent (dashed line) nebulization groups. Bars represent 1 SD.Figure 2. Clinical severity score changes for continuous (solid line) andintermittent (dashed line) nebulization groups. Bars represent 1SD. *P<.05 over baseline.S E P T E M B E R 2 0 0 0
A N N A L S O F E M E R G E N C Y M E D I C I N E
C O N T I N U O U S V E R S U S I N T E R M I T T E N T N E B U L I Z A T I O N O F S A L B U T A M O L
populations. Two studies by Moler et al27 and Portnoyand Aggarwal28 used an open-label design and were
In the present study, no appreciable difference was
uncontrolled. Both studies showed the efficacy and safety
observed between continuous and intermittent nebuliza-
of this nebulization modality. More recently, studies
tion of salbutamol in patients presenting to the ED with
including adult patients were performed to compare both
acute severe asthma in regard to spirometry (PEF), clini-
β -agonist nebulization modalities.13-18 Most of these
cal symptoms (clinical score), or disposition (hospitaliza-
studies were hampered by the wide variation in asthma
tion rate). However, this was a small study with limited
severity of the included patients, the limited duration of
power to detect differences in failure and hospitalization
the study, and evaluation of only spirometric improve-
rate. Accordingly, the decision to use intermittent or con-
ment. Overall, most of these studies did not document an
tinuous nebulization should be made on the basis of
additional benefit from continuous nebulization. When
logistical considerations (expense and nurse workload).
performing post hoc analysis on subsets of patients with
The dosage regimen of salbutamol used in this study
the most severe bronchial obstruction, Rudnitsky et al14
might appear quite high, especially in the light of findings
and Lin et al15 reported a superior effect of continuous
that two thirds of asthma attacks are terminated with
nebulization compared with intermittent nebulization.
doses as low as 2.4 to 3.6 mg of salbutamol from a metered-
The controlled study by Papo et al13 enrolled patients
dose inhaler20 and 5 to 7.5 mg from a nebulizer.8 How-
already hospitalized in a pediatric ICU with severe status
ever, it should be emphasized that the dosage regimen of
asthmaticus and found greater efficacy with continuous
the first hour (3 doses, 5 mg each) was in agreement with
β -agonist nebulization. Seventeen children with acute
the current international recommendations.1,2,5,7,8,21-23
severe asthma (Wood asthma score >5) were randomly
It should also be noted that no major side effects were
assigned to receive continuous or intermittent nebuliza-
observed in the present study and that with such a dosage
tion of salbutamol (0.3 mg/kg per hour). Efficacy criteria
regimen, serum levels of salbutamol are not elevated.5
consisted of the elapsed time to achieve a steady clinical
We elected to use a pneumatic nebulizer with a small
situation free from signs of impending acute respiratory
reservoir to avoid large amounts of residual volume, which
failure (Wood score <5 for at least 4 hours) and the need
can amount to as much as 20 mL when large nebulizers
for respiratory therapy. Continuous nebulization allowed
(60-mL) are used.15 An additional advantage of nebulizers
children to achieve more rapidly the assigned clinical
with small reservoirs is that they permit a double-blind
objective, shortened the duration of hospitalization, and
study by allowing the use of the same type of reservoir for
reduced the respiratory therapy time. However, the study
both continuous and intermittent nebulization.
by Papo et al was not blinded, had a too small sample size,
Most clinical trials dealing with acute asthma used
and the randomization process yielded a continuously
spirometric improvement as the main outcome measure.
treated group whose weight was 10 kg more than the
However, the change in pulmonary function is not
intermittent group, suggesting that the first group
directly related to clinical improvement and other rele-
received greater dosage of salbutamol.
vant outcome measures such as the rate of hospitalization
Continuous nebulization of β -agonists might be
or discharge from the ED.24 In the current study, we com-
expected to enhance the pulmonary function of patients
pared both nebulization modalities with spirometry, as
with acute asthma and ameliorate their clinical status more
well as change in clinical status and the rate of hospital-
rapidly than intermittent nebulization.13-15 These effects
ization. In addition, because the early physiologic and
should result in a reduced rate of hospitalization and the
clinical response to nebulized β -agonists has been
need for invasive procedures such as mechanical ventila-
recently shown to be an important factor in the prediction
tion or intravenous β -agonists. It has been speculated that
of the need of hospitalization and the potential for relapse,
these beneficial effects occur through an early deposition of
both nebulization modalities were compared with regard
β -agonists in the distal bronchi as bronchoconstriction is
to their rapidity of action, as expressed by the proportions
alleviated proximally and a sustained stimulation of pul-
of patients whose condition did not improve and required
monary β -adrenergic receptors, thereby preventing the
ICU admission by the first 40 minutes of the nebulization
rebound bronchospasm that might occur with intermittent
and the time interval needed to gain 3 points in the clini-
delivery.13 These effects might also be related to the high
blood levels of bronchodilators produced by continuous
The first publications on continuous nebulization of
nebulization of β -agonists, leading to synergistic effects of
β -agonists in acute asthma were conducted in pediatric
localized and systemic actions of β -agonists.29 However,
A N N A L S O F E M E R G E N C Y M E D I C I N E
S E P T E M B E R 2 0 0 0 C O N T I N U O U S V E R S U S I N T E R M I T T E N T N E B U L I Z A T I O N O F S A L B U T A M O L
Moler et al30 designed a controlled trial to address this
13. Papo MC, Frank J, Thompson AE. A prospective randomized study of continuous versus
issue and recorded similar levels of plasma terbutaline con-
intermittent nebulized albuterol for severe status asthmaticus in children. Crit Care Med. 1993;21:1479-1486.
centrations with both nebulization modalities, suggesting
14. Rudnitsky GS, Everlein RS, Schoffstall JM, et al. Comparison of intermittent and continu-
that the bronchodilator effects of β -agonists are not medi-
ously nebulized albuterol for treatment of asthma in an urban emergency department. AnnEmerg Med. 1993;22:1842-1846.
The lack of differences between both nebulization
15. Lin RY, Sauter D, Newmant T, et al. Continuous versus intermittent albuterol nebulization in
modalities observed in our study might be explained by
the treatment of acute asthma. Ann Emerg Med. 1993;22:1847-1853.
the fact that, at least in the first hour, these modalities are
16. Colacone A, Wolkove N, Stern E, et al. Continuous nebulization of albuterol (salbutamol) inacute asthma. Chest. 1990;97:693-697.
rather similar owing to the somewhat long half-life of
17. Shreshta M, Bidadi K, Gourlay S, et al. Continuous vs intermittent albuterol, at high and
salbutamol. In this regard, repeated nebulizations of
low doses, in the treatment of severe acute asthma in adults. Chest. 1996;110:42-47.
salbutamol at 20-minute intervals should be regarded as
18. Reisner C, Kotch A, Dworkin G. Continuous versus frequent intermittent nebulization of
almost identical to continuous nebulization. Our find-
albuterol in acute asthma: a randomized, prospective study. Ann Allergy Asthma Immunol. 1995;75:41-47.
ings of a nebulization time of approximately 12 to 13 min-
19. Weiss KB, Gergen PJ, Hodgson TA. An economic evaluation of asthma in the United States.
utes with an airflow of 6 to 7 L/min suggest that in the first
N Engl J Med. 1992;326:862-866.
hour, patients who receive an intermittent nebulization
20. Abroug F, Nouira S, Bchir A, et al. A controlled trial of nebulized salbutamol and adrenaline
remain without aerosol delivery for only a few minutes.
in acute severe asthma. Intensive Care Med. 1995;21:18-23.
These observations, together with the pharmacokinetic
21. Rodrigo C, Rodrigo G. Therapeutic response patterns to high and cumulative doses of salbu-
properties of a drug such as salbutamol (in particular, its
tamol in acute severe asthma. Chest. 1998;113:593-598.
half-life), should prompt consideration of a nebulization
22. McFadden ER Jr, Strauss L, Hejal R, et al. Comparison of two dosage regimens of albuterolin acute asthma. Am J Med. 1998;105:12-17.
strategy consisting of 1 dose every 20 minutes as quite
23. Emerman CL, Cydulka RK, McFadden ER. Comparison of 2.5 vs 7.5 mg of inhaled albuterol
in the treatment of acute asthma. Chest. 1999;115:92-96.
24. Fischl MA, Pitchenik A, Gardner LB. An index predicting relapse and need for hospitalization
We appreciate the review of the manuscript by Professor Laurent Brochard (Creteil,
in patients with acute bronchial asthma. N Engl J Med. 1981;305:783-789.
France). We also thank the physicians and nurses of the emergency department of F. Bourguiba Hospital, without whom this study would not have been possible.
25. Rodrigo G, Rodrigo C. A new index for early prediction of hospitalization in patients withacute asthma. Am J Emerg Med. 1997;15:8-13.
26. Rodrigo G, Rodrigo C. Early prediction of poor response in acute asthma patients in the
emergency department. Chest. 1998;114:1016-1021.
National Asthma Education and Prevention Program. Expert Panel Report 2: Guidelines for
27. Moler FW, Hurwitz ME, Custer JR. Improvement in clinical asthma score and PaCO2 in chil-
the Diagnosis and Management of Asthma [NIH publication No. 97-4051]. Bethesda, MD:
dren with severe asthma treated with continuously nebulized terbutaline. J Allergy Clin
National Institutes of Health; July 1997.
The British Guidelines on Asthma Management. 1995 review and position statement.
28. Portnoy J, Aggarwal J. Continuous terbutaline nebulization for the treatment of severe
Asthma in adults and school children. Thorax. 1997;52:S2-S8.
exacerbation of asthma in children. Ann Allergy. 1988;60:368-371.
Rossing TH, Fanta CH, Goldstein DH, et al. Emergency therapy of asthma: comparison of
29. Lin RY, Smith AJ, Hergenroeder P. High serum albuterol levels and tachycardia in adult
the acute affects of parenteral and inhaled sympathomimetics and infused aminophylline. Am
asthmatics treated with high-dose continuously aerosolized albuterol. Chest. 1993;103:221-225. Rev Respir Dis. 1980;122:365-371.
30. Moler FW, Johnson LE, Van Laanen C, et al. Continuous versus intermittent nebulized
High-dose inhaled versus intravenous salbutamol combined with theophylline in severe
terbutaline: plasma levels and effects. Am J Respir Crit Care Med. 1995;151:602-606.
acute asthma. Swedish Society of Chest Medicine. Eur Respir J. 1990;3:163-170.
31. Jenne JW, Ahrens RC. Pharmacokinetics of beta-adrenergic compounds. In: Jenne JW,
Salmeron S, Brochard L, Mal H, et al. Nebulized versus intravenous salbutamol in hypercap-
Murphy S, eds. Drug Therapy for Asthma: Research and Clinical Practice. New York, NY: Dekker;
nic acute asthma. A multicenter double blind randomized study. Am J Crit Care Med.
Browne GJ, Penna AS, Phung X, et al. Randomised trial of intravenous salbutamol in early
management of acute severe asthma in children. Lancet. 1997;349:301-305.
McFadden ER, Elsanadi N, Dixon L, et al. Protocol therapy for acute asthma: therapeutic
benefits and cost savings. Am J Med. 1995;99:654-661.
Strauss L, Hejal R, Galan G, et al. Observation on the effects of aerosolized albuterol in
acute asthma. Am J Respir Crit Care Med. 1997;155:454-458.
Peake JE, Mellon AF. Asthma guidelines, burst therapy for acute asthma [letter, comment].
10. Nelson HS, Spector SL, Witsset TL. The bronchodilator response to inhalation of increasingdoses of aerosolized albuterol. J Allergy Clin Immunol. 1983;72:371-375.
11. Britton J, Tattersfield A. Comparison and noncumulative techniques to measure dose-response curves for beta agonists in patients with asthma. Thorax. 1984;39:597-599.
12. Roberston CF, Smith F, Beck R. Response for frequent low doses of nebulized salbutamol inacute asthma. J Pediatr. 1985;106:672-674. S E P T E M B E R 2 0 0 0
A N N A L S O F E M E R G E N C Y M E D I C I N E
O Summe L r 2003 OGY ROBOTIC RADICAL PROSTATECTOMY COMES TO DUKE Even though radical prostatectomy remains the goldprocedure is performed in the same way as the LRP butstandard for the treatment of localized prostate cancer, thewith the assistance of a daVinci robotic surgical systemradical retropubic prostatectomy (RRP) and radical per-(Intuitive Surgical, Inc., Mountain View,
COMMISSION REGULATION (EC) No 407/2009 of 14 May 2009 amending Council Regulation (EC) No 338/97 on the protection of species of wild fauna and flora by regulating trade therein THE COMMISSION OF THE EUROPEAN COMMUNITIES, Bolitoglossa dofleini, Cynops ensicauda, Echinotriton andersoni, Pachytriton labiatus, Paramesotriton spp., Salamandra algira and Tylototriton spp. – which a
 C O N T I N U O U S V E R S U S I N T E R M I T T E N T N E B U L I Z A T I O N O F S A L B U T A M O L
C O N T I N U O U S V E R S U S I N T E R M I T T E N T N E B U L I Z A T I O N O F S A L B U T A M O L