Endodontic Topics 2002, 3, 52–66Copyright C Blackwell MunksgaardPrinted in Denmark. All rights reservedENDODONTIC TOPICS 2002 Are antibiotics effective for endodontic pain? An evidence-based review
Although antibiotics are frequently prescribed to treat endodontic pain patients, there is little evidence fromthe clinical literature to support this indication. This review focuses on the clinical evidence regarding theefficacy of antibiotics for treating postendodontic pain.
Antibiotics are frequently prescribed to aid in the
chemokines, kinins, serotonin, and neuropeptides are
treatment of endodontic pain. Over the past 25 years,
produced during the inflammatory process. These in-
several surveys of general dentists and endodontists
flammatory mediators activate or sensitive nocicep-
have been conducted that illustrate a persistent pat-
tors terminating in the pulp, the periodontal ligament
tern of prescribing antibiotics in conjunction with en-
or periradicular bone, induce sprouting of nocicep-
dodontic treatment (1–5). However, despite concur-
tors (leading to increased receptivity to stimuli), and
rent advances in our understanding of the biology of
evoke edema and increased tissue pressure by increas-
inflammatory and infectious processes, and the in-
ing vascular permeability in these tissues.
creased awareness of the side-effects of antibiotics,
The ability of an antimicrobial medication to effec-
most notably the emergence of resistant bacterial
tively reduce pain occurring during these inflamma-
strains, there seems to be little change observed in
tory conditions is not clear. A spreading infection of
the practice of prescribing antibiotics.
endodontic origin may be painful, particularly if there
This review focuses on the effects of antibiotic
is excessive increase in pressure within the tissues.
medications for reducing postendodontic symptoms,
However, the pain is a result of the inflammatory re-
primarily pain. This paper is not intended to be a re-
action that accompanies the infectious process. Inter-
view of endodontic microbiology, and the general
ventions that reduce this inflammatory process (e.g.
pharmacology of antibiotics. The reader is referred to
direct elimination of the microbial irritants by chemo-
a number of excellent recent reviews on this topic (6–
mechanical debridement of the root canal system, in-
10). Rather, the clinical studies to be reviewed focus
cision and drainage of a purulent swelling, or extrac-
on the efficacy of antibiotics, mostly in conjunction
tion of an unrestorable tooth) are effective at reduc-
with non-surgical endodontic treatment, for treating
ing pain. However, there is considerable debate in the
postoperative signs and symptoms of endodontic pa-
literature as to whether the additional prescription of
Endodontic pain is the result of an inflammatory
Occasionally, the inflammation is related to a
process, which is most commonly related to microbial
spreading infection where the host responses do not
irritation but which may also be related to mechanical
appear to be capable of controlling the spread of mi-
or chemical factors. A variety of chemical mediators
crobial factors. In these cases antibiotics are usually
such as arachidonic acid metabolites, cytokines,
prescribed in addition to the local treatment to aug-
ment host response mechanisms. It is important for
levels in bone peaked at 6.33 mg/g, with a bone to
clinicians to know, given the side-effects of anti-
serum mean ratio of 0.2 (11). Using the same meth-
biotics, whether the benefits of prescribing antibiotics
odology, these investigators were able to study the
in conjunction with standard endodontic treatment
levels of bacampicillin in periapical granulomas, rad-
methods outweigh the risks involved. This review will
icular cyst walls and cyst fluids (14, 15). The granu-
address only cases with preexisting pulpal or periradic-
loma to serum, cyst wall to serum and cyst fluid to
ular pain. For a review of the subject of whether anti-
serum mean ratios were 0.42, 0.23 and 0.77, respec-
biotics can be used prophylactically to prevent post-
tively. They also showed that while the concentrations
operative pain, the reader is referred to the article by
in granulomas may differ between ampicillin and a
R. Walton in this issue of Endodontic Topics.
macrolide antibiotic (josamycin), the levels may ex-
To review this topic, we have addressed seven speci-
ceed the minimum inhibitory concentration (MIC)
fic issues of antibiotics that relate to their ability to
of some endodontic bacteria for the former and the
alter postendodontic pain or infection.
MIC80 for the latter (16, 17). Another study showedthat even within the macrolide class of antibiotics,
1) Can systemically administered
erythromycin acistrate had much higher levels in
antibiotics reach pulpal and
plasma and in periradicular lesions compared with
periradicular tissues in therapeutic
erythromycin stearate when both drugs were given 2–
concentrations?
6 days before an apicoectomy (18). Four commonlyprescribed antibiotics were compared as to their levels
Antibiotic effectiveness is related to both the type and
in serum and periapical exudates from induced peri-
concentration of the antibiotic. Clearly, if antibiotics
apical lesions in dogs (19). In this study, the mean
are to be effective in managing endodontic infections
ratio of peak lesion/serum antibiotic concentration
and reducing endodontic symptoms, they must reach
was lowest for benzylpenicillin (0.4 at 1 h) followed
the target tissues in therapeutic concentrations. This
by erythromycin (0.75 at 1 h), clindamycin (0.96 at
is especially a concern in pathological conditions,
4 h), and lincomycin (1.07 at 4 h). The last two anti-
when the tissues may have reduced blood flow or may
biotics had better permeation of periradicular lesions
but had a later peak concentration. Taken together,
In a study on the vital dental pulp from patients
these studies show that antibiotics can permeate vital
with impacted or partially erupted mandibular third
pulpal and periradicular tissues within hours in levels
molars, it was shown that the levels of an ampicillin
that can reach MIC for some pathogens, but that per-
analog (bacampicillin 250 mg oral) peaked in the pulp
meation of empty pulp space may take days, and is
in about 90 min and reached a concentration of 16.7
mg/g (11). The mean ratio of antibiotic in the pulpto that in serum at peak values was 0.61, with a range
2) Are systemic antibiotics effective
of 0.01–0.99. Another study was done on dogs, to
for treating pulpal pain?
measure the bioavailability of ampicillin in the pulpspace of teeth in which the pulp had been extirpated
Painful irreversible pulpitis is effectively managed by
(12). The animals were maintained on ampicillin 500
pulpotomy or pulpectomy (20). In a survey con-
mg i.m. every 12 h, and a bioassay was used to
ducted in 1990, the percentage of board-certified en-
measure zones of inhibition of a microorganism sensi-
dodontists who would prescribe antibiotics for pa-
tive to ampicillin. The antibiotic was first detected in
tients with irreversible pulpitis was 4–15% (depending
half the samples at 3 h following the first injection.
upon the presence of acute apical periodontitis) (3).
About 80% of the teeth had inhibitory concentrations
Another survey conducted 10 years later on all mem-
by the first day, and all had the same result by 3 days.
bers of the American Association of Endodontists
The mean levels of the antibiotics bacampicillin,
showed an almost identical pattern of prescribing
clindamycin, erythromycin, and doxycycline in bone
antibiotics in these conditions, where the percentages
were measured in patients undergoing third molar ex-
were 3.5% and 13.2%, respectively (4). The infectious
tractions, and were found to be lower than in other
process in these cases is localized within the pulp, and
oral tissues (11, 13). For example, the bacampicillin
the pain is most probably caused by the actions of
inflammatory mediators on peripheral nociceptive
in the last 25 years. However, there is a clear trend in
neurons (21, 22). However, the specific response
these studies that endodontists are more inclined to
within the pulp to bacteria in deep caries has been
prescribe antibiotics in cases with pulp necrosis if
documented (23, 24), together with the increase in
symptoms with certain bacterial species (25).
Therefore, a prospective, randomized, double-
O endodontic treatment is not associated with signifi-
blind, placebo-controlled study was recently con-
ducted to determine the effect of penicillin on pain
in untreated teeth, diagnosed with moderately to se-
O if the swelling is visible extra-orally.
verely painful irreversible pulpitis (26). The outcome
In treating periradicular pathosis of an acute nature,
variables were the differences in spontaneous pain and
the objectives are to control the spread of the infec-
percussion pain between the penicillin and the pla-
tion and to obtain expedient relief of symptoms. It is
cebo groups after 7 days, as well as the amount of
universally accepted that the main emphasis in treat-
analgesic medications used by both groups during
ment is on the removal of the cause, which in this
this period. Importantly, this study revealed no statis-
case would be the debridement of the necrotic pulp
tically significant results between the two groups on
tissue and disinfection of the root canal space or ex-
any of the parameters evaluated, indicating, quite
traction of unrestorable teeth. Incision for drainage is
convincingly, that antibiotic use does not relieve pain
also indicated for elimination of purulent discharge.
due to irreversible pulpitis. In other words, antibiotic
It is also known from a number of studies that pa-
usage produced the same responses as that seen in
tients presenting with pretreatment pain (27–29),
patients given an inert placebo tablet.
particularly periradicular pain (29), are more likely toexperience interappointment flare-ups. Therefore, in
3) Are antibiotics effective for
evaluating the effectiveness of antibiotics on the relief
resolving localized periradicular
of periradicular symptoms in these cases, the underly-
symptoms?
ing premise is that the elimination of the local irri-tants is the main focus of treatment. That leaves the
Table 1 shows the main findings from three surveys
following debatable question: how much can the pre-
conducted among endodontists regarding the issue of
scribing of antibiotics enhance and expedite the pro-
prescribing antibiotics. The surveys show that most
cess of symptom relief, beyond what could be ob-
endodontists prescribe antibiotics for patients with
tained by performing the same treatment without
necrotic pulp and periradicular pain, and that this
finding does not appear to have changed significantly
The focus in this section will be to address cases
Table 1. Trends in antibiotic prescribing for periradicular (PR) pain among endodontists
Pulp necrosis with PR pain, and localized swelling
Pulp necrosis with PR pain, and diffuse swelling
‡For pulp necrosis with acute apical periodontitis, with swelling and with moderate to severe pain, 99.21% of respondents in this study would prescribe antibiotics. *Cases with drainage obtained through the canal. †No extra-oral swelling. §With extra- oral swelling. Table 2. Effect of antibiotics used to augment endodontic procedures in resolving periradicular symptoms
Acetaminophen π codeineIbuprofen π penicillinIbuprofenKetoprofenPenicillinErythromycin baseMethylprednisolone π penicillin
Ketoprofen (6, 12, 18, 24, 48)Penicillin (18, 24, 30, 36, 42,48, Ͼ48)Erythromycin base (6, 12, 18,24, 30, 36, 42, 48, Ͼ48)Methylprednisolone πpenicillin(6, 18, 24)
*Patients in the instrumentation phase of the study with moderate to severe preoperative pain; it is not clear how many patientsin the obturation phase were in pain prior to obturation. †Numbers are time points in hours when medications were foundto be effective. ‡Patients in all three groups were given ibuprofen for 24 h.
with pulp necrosis with localized periradicular symp-
mycin base 50 mg qid (ERYC, Parke-Davis, Morris
toms. Table 2 summarizes the main features of four
Plains, NJ, USA). In fact, ERYC was the most effec-
prospective, randomized, double-blind clinical trials
tive medication in patients who were in moderate to
that have addressed this issue (30–33). These studies
severe pain preoperatively, since it was significantly
were all in agreement that there was a statistically sig-
more effective than placebo at the highest number of
nificant reduction in periradicular symptoms follow-
time points. However, this study included patients
ing conventional chemomechanical instrumentation
with different pulpal and periradicular diagnoses, and
in all groups, including the controls that received pla-
the percentage of patients with pulp necrosis and peri-
cebo or no medications. In the study by Torabinejad
radicular radiolucencies was much lower in the pla-
et al. (33), further benefit was shown for the use of a
cebo group than in the penicillin and erythromycin
number of postoperative medications (Table 2), in-
groups. Pulp vitality and lack of a periradicular radio-
cluding two antibiotics: penicillin 500 mg qid (Veet-
lucency were, more recently, shown to be significant
ids, Apothecon, Princeton, NJ, USA) and erythro
factors in postoperative pain experience (34), where
patients in these groups were more likely to benefit
periradicular infection may or may not be associated
from occlusal reduction than patients with pulp ne-
with a localized swelling, depending on whether the
crosis or with periradicular radiolucency. Further-
cortical plate had been sufficiently resorbed for the
more, the percentages of patients who were prema-
infection to reach the periosteum or the mucosal
turely terminated from the study because they experi-
tissues. However, the conditions both with and with-
enced an increase in symptoms and needed other
out swelling could be considered different stages of
medications, were comparable among the placebo,
the same disease that could be managed primarily by
penicillin and erythromycin groups (11.3%, 7% and
local therapeutic measures (which may include the
10.9%) (33). When postobturation pain was studied
drainage of a swelling as well as canal debridement
in the same cohort of patients, there were no statisti-
cally significant differences among the medications
Conversely, spreading infections indicate that bac-
teria have traveled to sites distant from the original
In the two subsequent studies (30, 31), only pa-
source of infection, and are virulent enough to invade
tients with pulp necrosis, periradicular radiolucencies
tissues and cause significant morbidity and even mor-
and periradicular pain were included, in order to con-
tality (35–38). Spreading infections are associated
trol for these important variables. It is difficult to
with findings such as extra-oral swelling, fascial space
examine the effects of antibiotics on patients with
involvement, fever, malaise, significant submandibular
pain without prescribing analgesic medications, which
and cervical lymphadenopathy, muscle trismus, pain
are known to relieve discomfort. Therefore, both
during swallowing and other respiratory or neuro-
studies controlled for this variable in different ways.
logical disorders. Fever is usually above 100 æF (or
In the first study, patients in all groups were given
37.7 æC) and may or may not be associated with leu-
ibuprofen 600 mg every 6 h for 24 h, then as needed
kocytosis and increased sedimentation rate (9, 39).
(30), whereas in the second study, the NSAID and
While many infections associated with signs and
the narcotic medications were given to the patients
symptoms of systemic involvement are successfully
with instructions on when and how to use them. The
managed by general dentists and endodontists, the
unused tablets were then counted and the data used
more serious cases are usually referred to oral and
as another dependant variable (31). The findings of
maxillofacial surgeons, as they may involve extensive
both studies were consistent in showing that patients
surgical drainage procedures and hospitalization of
with pulp necrosis and localized acute apical symp-
the patient. Again, the main emphasis in treatment is
toms had significant improvement of their condition
on the removal of the etiologic source of the infec-
following conventional cleaning and shaping of the
tions at the primary site or invaded tissues, as well
root canal system, and that the use of penicillin did
as supportive measures that include treatment with
In the study by Torabinejad et al. (33), it was
The effectiveness of antibiotics in the management
shown that not only the presence of preoperative
of significant infections can be assessed by examining
pain, but also preoperative apprehension was associ-
the results of culture and sensitivity studies on bac-
ated with postoperative pain. This illustrates the im-
teria involved in odontogenic infections, and by
portance of controlling for as many treatment vari-
examining the few clinical trials that have compared
ables as possible in determining post-treatment out-
different antibiotics in the management of these in-
fections. For sensitivity testing, a bacteriologicalsample is obtained and cultured under aerobic and
4) Are antibiotics effective in cases
anaerobic conditions. Testing may be done by the dif-
with significant odontogenic
fusion method where disks impregnated with the
infections?
antibiotic are placed on blood agar plates inoculatedwith the test organism, and the zone of inhibition
As was mentioned before, it is essential to distinguish
surrounding the disk is measured. However, this
between two different forms of acute periradicular
method is not reliable for strict anaerobic organisms
symptoms associated with pulp necrosis, namely, lo-
that need long incubation periods (40). Another
calized and spreading infections. The painful localized
method for microbial sensitivity testing is the dilution
method, where serial dilutions of common antibiotics
acterized by skin fistulae and the production of yel-
are inoculated with the test organism to determine
lowish granules (55). Actinomyces israelii, which is
the minimum inhibitory concentration (MIC) for
thought to have the ability to survive in soft tissues
each antibiotic. MIC is the lowest concentration of
forming the classic actinic ray colonies, is sensitive to
the antibiotic that will inhibit visible growth in vitro.
penicillin, administered for extended durations of 2–
MIC can be used to determine the minimum bacteri-
6 weeks (56). However, actinomycosis must be diag-
cidal concentration (MBC), by incubating established
nosed by its classic clinical features or through a bi-
subcultures of the sensitive organism with different
opsy, since the indiscriminate long-term use of peni-
dilutions of the antibiotic overnight. The antibiotic is
cillin not only may lead to side-effects (see below) but
considered bactericidal when the MBC is equal to or
is not effective in improving long-term healing of
less than fourfold higher than the MIC (40).
cases with routine endodontic infections (57).
Antibiotic sensitivity testing plays a limited role in
The results of a number of studies that compared
most clinical cases of endodontic infections; it is gen-
the effectiveness of different oral antibiotic in the
erally employed when a significant infection appears
treatment of odontogenic infections are shown in
to be resistant to the antibiotics prescribed on an em-
Table 3 (58–62). In general, the different antibiotics
pirical basis, in patients who are significantly immuno-
used were ones that had been shown to be effective
compromised or in infections that are considered very
against most odontogenic bacteria from culture and
serious in nature. Because antibiotic testing is a slow
sensitivity testing, namely, penicillin, amoxycillin,
process, patients are frequently started on empirical
clindamycin, cephalosporins and augmentin, which
antibiotics while the results of sensitivity testing are
combines amoxycillin with clavulanic acid, the latter
being effective against penicillin-resistant organisms.
As early as 1962, Goldman & Pearson (41) recog-
With the exception of the faster improvement in con-
nized that a number of microorganisms cultured from
stitutional symptoms by cephradine (a first generation
the necrotic pulp specimens are resistant to penicillin.
cephalosporin) in one study (62), and faster reduc-
Nevertheless, a large number of antibiotic sensitivity
tion in pain by augmentin in another study (61), all
studies performed on necrotic pulp specimens or
the medications tested appear to be of similar efficacy.
aspirates from odontogenic abscesses have shown that
It is difficult to assess the overall effectiveness of anti-
penicillin remains the primary antibiotic of choice for
biotics in these studies since they did not include
endodontic infections, followed by clindamycin or
groups that received surgical drainage alone or with a
erythromycin as alternative choices (42–46). In a re-
cent series of studies on a relatively large number of
The choices of penicillin (or amoxicillin) as the pri-
odontogenic infections, it was shown that most of the
mary antibiotic prescribed, and clindamycin as the
microorganisms identified were susceptible to b-lac-
drug of second choice appear to be consistent with
tam antibiotic, most notably penicillin. A small per-
choices made by dentists or endodontists on recent
centage of organisms produce b-lactamase, and were
surveys, although some dentists seem to favor ery-
members of the Prevotella and Staphylococcus genera
thromycin for patients with penicillin allergy (4, 5).
(44, 47, 48). As would be expected, the incidenceof b-lactamase-producing bacterial strains was much
5) Are locally applied antibiotics
higher in patients with past history of b-lactam anti-
effective for treating pain?
biotic use (44, 49). b-lactamase-positive organismswere sensitive to clindamycin (48) and some b-lactam
Numerous antimicrobial agents have been used to
antibiotics such as the cephalosporins cefmetazole or
eliminate bacteria or bacterial products locally from
cefoperazone/sublactam, imipenem, and faropenem
the root canal system. These agents have been used
primarily as irrigants that can be used during root ca-
In the discussion of antibiotics and periradicular in-
nal instrumentation, or pastes, gels or impregnated
fections it is important to note that Actinomyces spp.
solid fillers that can be used as interappointment
have been detected in chronic periradicular lesions in
medicaments. There has always been a quest to dis-
a number of studies (51–54). Cervico-facial actino-
cover an agent that has potent, broad-spectrum anti-
mycosis is a more aggressive form of the disease char-
microbial properties, yet is relatively non-toxic. Anti-
biotics have been historically attractive from this per-
doxycycline hyclate in a gel delivery system (Atri-
spective because of their specific antibacterial actions
dox, Collagenex, Newtown, PA, USA), and mino-
and their low degree of toxicity for mammalian cells.
The use of antibiotics in a locally applied manner
Warminster, PA, USA). Therefore, it is prudent to
could potentially provide the antimicrobial prop-
review the use of locally delivered antibiotics in
erties in sufficient doses for as long as is needed,
endodontics, and whether they could contribute to
without having the undesirable systemic side-effects.
Although the systemic use of some antibiotics has
Antibiotics are generally effective during the repro-
been shown to allow the diffusion of these medi-
ductive cycle of the bacterial cells and thus would not
cations into the root canal space in animal models
be suitable for short-term use as an irrigating solution
(12, 19), the local application would offer the sus-
(66). The use of certain antibiotics such as tetracy-
tained and concentrated presence of the medication
cline-HCl as endodontic irrigants may have another
to potentially allow more effective bacterial elimin-
benefit, which is the removal of smear layer, thereby
ation. There is also a growing interest in local deliv-
allowing better cleansing of the root canal system
ery of antibiotics to augment conventional treat-
(67). However, for antimicrobial use, which is what
ment of periodontal patients with refractory forms
could potentially reduce bacterial irritation and endo-
of advanced marginal periodontitis (63–65). In the
dontic symptoms, antibiotics have been generally
past decade, the Food and Drug Administration
used as interappointment medicaments. It should also
has approved three different formulations for locally
be stated that in the earlier studies on the use of anti-
delivered antibiotics for periodontal use. These are
biotic pastes in root canals, the emphasis was on the
tetracycline-HCl in an ethylene/vinyl acetate co-
total elimination of cultivable bacteria from the root
polymer controlled release periodontal fiber (Actis-
canal prior to obturation, rather than other require-
ite, ALZA Laboratories, Palo Alto, CA, USA), 10%
ments such as symptoms or long-term healing. Table 3. Double-blind studies comparing differences in effectiveness of currently available oral antibiotics, pre- scribed for significant odontogenic infections. These studies did not have groups with placebo or no medications
Fazakerley et al. 1993 (62) Lewis et al. 1993 (61)
first aid antimicrobial ointments, is not specific for
Sulfonamides
endodontic bacteria and is therefore not considered
Sulfonamides are synthetic bactericidal antimicrobial
agents that affect the synthesis of folic acid by inter-
The danger of superinfections with resistant bac-
fering with the bacterial update of para-aminobenzoic
teria, the risk of sensitization or allergic reactions and
acid (PABA) because they are structurally similar.
the difficulty in obtaining some formulations are
They are specific for gram-positive bacteria, but re-
probably the main reasons for the diminished use of
sistance to them develops frequently (68). Sulfanilam-
polyantibiotic root canal medicaments.
ide and sulfathiozole (69) were used in the past asroot canal medicaments, presumably because strepto-
Ledermix
cocci were the main organisms cultured from root ca-nals at the time. As early as 1945, Dr. Louis
Ledermix is a paste that combines 1% triamcinolone
Grossman published a study in which blinded oper-
acitonide (a corticosteroid) and demethylchlorotetra-
ators placed these sulfonamide preparations or a con-
cycline (demeclocycline, a tetracycline analog). It has
trol as interappointment medicaments. Comparisons
been used as a pulp capping agent, and as a root canal
were made on the number of appointment needed for
medicament for both vital and necrotic cases because
negative cultures, and sulfonamides were inferior to
of its anti-inflammatory and antimicrobial properties
other medicaments used at the time in all diagnostic
(66). Both components of Ledermix can diffuse into
categories evaluated (70). Furthermore, sulfonamides
dentin and through the apical foramen (75). The con-
tend to cause yellowish tooth discoloration (69) and
centration of demeclocycline in the root canal was
therefore are no longer used in this application.
shown to be much higher than is required to inhibitbacteria; however, this activity tends to decrease con-siderably by 7 days (66). It may be combined with
Penicillin-bacitracin-streptomycin-sodium
calcium hydroxide at a 50 : 50 ratio to enhance its
caprylate (PBSC)
antimicrobial efficacy, but this tends to reduce the dif-
This polyantibiotic paste was introduced and evalu-
fusion of its main ingredients (76).
ated by Dr. Grossman in 1951 (71). Penicillin (1 000
Ledermix was shown to be efficacious against pul-
000 U) interferes with cell wall synthesis of actively
pal pain in some earlier studies (77), possibly because
multiplying gram-positive bacteria and a few gram-
of its corticosteroid content; however, pulp capping
negative anaerobes. Bacitracin (10 000 U) is also bac-
for painful cases with pulp exposures is not currently
tericidal against gram-positive bacteria and was in-
recommended because of its low long-term prognosis
cluded to target bacteria resistant to penicillin. Strep-
(78). In a randomized clinical trial to compare Leder-
tomycin (1 g) is bacteriostatic against gram-negative
mix with formocresol and calcium hydroxide used as
facultative anaerobes and sodium caprylate (1 g)
interappointment medicaments on postinstrumen-
against Candida. Nystatin replaced sodium caprylate
tation flare-ups, no differences were detected among
in another formulation (69). Despite the finding in a
later study that no detectable penicillin was absorbedsystemically (72), a few cases have been reported with
Clindamycin
allergic reactions to penicillin following its adminis-tration through the root canal system (73).
There have been some trials evaluating clindamycin
Other polyantibiotic combinations were marketed,
as an intracanal medicament. Clindamycin is a potent
primarily in Europe and Australia, in which penicillin
bactericidal antibiotic that binds to the 50S ribosomal
was replaced with less allergenic antibiotics (66, 74).
subunit and interferes with protein synthesis (68).
Septomixine Forte is one formulation, which was pri-
However, systemic administration of clindamycin is
marily composed of neomycin sulfate, an aminogly-
associated with the occasional occurrence of diarrhea,
coside active against many gram-negative organisms,
and the uncommon, potentially serious, condition
and Polymyxin B sulfate, which is bactericidal for a
pseudomembranous colitis caused by overgrowth of
variety of gram-negative organisms. This combi-
Clostridium difficile. Therefore, local application of
nation, which is now common in a lot of the OTC
the drug might be advantageous to minimize these
systemic side-effects. In a clinical study, clindamycin
term macrolides for chronic conditions such as
was shown to be comparable to calcium hydroxide in
asthma have improvements of their clinical symptoms
eliminating bacteria from root canals, and also in
due to nonantibiotic properties of the drugs (82, 83).
being not effective against enterococci (80). Recently,
Recently, controlled clinical trials have shown that
clindamycin-impregnated ethylene vinyl acetate fibers
chronic diseases such as panbronchiolitis and cystic
were investigated in vitro and found to be effective
fibrosis treated with macrolides show a decrease in
against other common endodontic pathogens (81).
disease parameters and an improvement of the inflam-
This fiber has the advantage over the tetracycline fiber
Actisite mentioned before, in that it does not discolor
A number of studies have been conducted to ex-
teeth. However, further investigations of this fiber in
plain the mechanisms whereby macrolides exert these
clinical situations have not been reported.
anti-inflammatory actions. Using the rat carrageeninpaw edema model, roxithromycin given prophylac-
6) Do certain antibiotics have anti-
tically suppressed edema produced by injecting carra-
inflammatory properties?
geenin into the paw at levels comparable to those ofthe non-steroidal anti-inflammatory drug nimesulide
Clearly, the main reason for using antibiotic therapy
(86). Azithromycin and clarithromycin also had po-
in conjunction with endodontic therapy is to reduce
tent anti-inflammatory effects in that study while ery-
or eliminate bacteria, thereby reducing the infectious
thromycin had the least anti-inflammatory effects.
process. If an endodontic infection is associated with
These macrolides also reduced prostaglandin E2 and
pain, and if the antibiotic happens to be effective
TNF-a in pleural exudate when carrageenin was in-
against the bacterial pathogens involved and reaches
jected in the pleural cavity, with roxithromycin again
the infection site in therapeutic concentrations, it is
being the most effective (87). In an in vitro study,
anticipated that the irritants will be eliminated and
these macrolides (except for azithromycin) stimulated
the inflammatory process will be reduced, resulting
macrophage growth, and (except for roxithromycin)
in pain resolution. Analgesic and anti-inflammatory
stimulated macrophage phagocytosis, chemotaxis to
medications work in a more direct and expedient
lipopolysaccharide (LPS), and cytocidal activity
manner to reduce inflammatory mediators or reduce
against Candida albicans (88). The same four macro-
hyperalgesia either centrally or peripherally, and thus
lides were also shown to cause a dose-dependent inhi-
are the preferred medications for immediate pain re-
bition of superoxide production by activated neutro-
lief. However, recently, a number of anti-inflamma-
phils (89). It was recently demonstrated that rox-
tory properties have been attributed to certain anti-
ithromycin does not inhibit mast cell growth or its
biotics that appear to be unrelated to their anti-
ability to produce histamine, but suppresses this cell’s
microbial functions. In the discussion of the effect of
ability to produce the cytokines IL-1b, IL-6, GM-
antibiotics on pain, it is important to address these
CSF and TNF-a when stimulated by concanavalin A
properties as they may contribute in a direct way to
(90). Erythromycin was shown to reduce the cyto-
the mechanisms of effectiveness of antibiotics at the
kine-evoked production of chemotactic factors eo-
site of endodontic pain, and may influence the choice
taxin and RANTES from a human lung fibroblast cell
of an antibiotic medication, if one is indicated.
line (91), and modulate the production of the chemo-kine IL-8 from alveolar macrophages (92).
These anti-inflammatory properties of macrolides
Macrolides
have not been explored in the endodontic literature.
Macrolides are bacteriostatic antibiotics that exert
However, erythromycin in particular has been investi-
their action by interfering with bacterial protein syn-
gated in a number of studies as to its antimicrobial
thesis by binding to the 50S ribosomal subunit, it is
efficacy, although the use of erythromycin for endo-
thought by binding to the donor site during the
dontic reasons has recently diminished because of its
translocation step (68). Among the more commonly
documented gastrointestinal side-effects (93, 94). In
prescribed macrolides are erythromycin, clarithromy-
the multicenter trial by Torabinejad et al. discussed
cin, azithromycin and roxithromycin. It has been ob-
before, it was found that erythromycin was the most
served for some time that patients treated with long-
effective of a group of nine drugs or drug combi-
nations in reducing moderate to severe symptoms fol-
treatment of patients and global public health issues.
lowing root canal instrumentation (33) (Table 2).
Among the well-documented side-effects to anti-
Erythromycin was also significantly more effective
biotics commonly prescribed for endodontic infec-
than the other medications in reducing postobtu-
tions are hypersensitivity reactions and drug fevers to
ration pain in the same cohort of patients; however,
penicillin and other b-lactam antibiotics, pseudo-
the difference disappeared when preobturation pain
membranous colitis, which occasionally occurs with
was accounted for (32). As was mentioned before,
clindamycin or other antibiotics, nausea, vomiting
these studies had a number of variables that were not
and gastrointestinal distress common with macro-
clearly defined, making it difficult to draw direct con-
lides, photosensitivity that may accompany tetracy-
clusions. However, in light of the medical findings,
cline and renal toxicity that may be associated with
the role of newer macrolides in endodontic sympto-
matic infections should be further explored.
Hypersensitivity side-effects are more common
among b-lactam antibiotics, and while drug rash,serum sickness and anaphylactic reactions are well rec-
Tetracyclines
ognized by clinicians, drug fevers are the most com-
Tetracyclines are another group of bacteriostatic anti-
mon antibiotic-mediated hypersensitivity side-effect
biotics that bind to the 30S ribosomal subunit of bac-
(102). Drug fevers account for 10–15% of unex-
plained fevers in hospitalized patients in the U.S., and
aminoacyl-t-RNA synthetases to the ribosomal ac-
may occur with any medication, but are common
ceptor site (68). A number of beneficial nonanti-
with b-lactams and sulfonamides (102). Gastrointesti-
microbial properties have been described for tetracy-
nal side-effects are common among many medi-
clines and tetracycline analogs, even when used in su-
cations, but in particular macrolide antibiotics. Clar-
bantimicrobial doses. The most important of these
ithromycin (such as Biaxin XL) and azithromycin are
properties is the inhibition of expression and produc-
associated with less GI irritation than erythromycin
tion of host matrix metalloproteinases (MMPs) (95–
(103). Diarrhea is a frequent symptom of GI distress
97). MMPs are a group of 11 or more endopeptidases
in patients on macrolides, b-lactams or clindamycin,
that include collagenases, gelatinases and other en-
and may be a direct irritation of the intestinal mucosa
zymes that are up-regulated during inflammation,
or an imbalance in intestinal flora. As was noted be-
causing tissue destruction (98). It was recently shown
fore, one type of complication of antibiotics due to
that levels of MMP-9 (a gelatinase) were significantly
the microbial imbalance is the overgrowth of Clostri-
higher in inflamed than in normal dental pulps (99). dium difficile, causing pseudomembranous colitis, a
Tetracycline is also thought to inhibit osteoclasts,
rare but serious condition. This condition can de-
thereby reducing bone resorption, and can act syner-
velop up to 6 weeks after cessation of therapy (103),
gistically with other agents that reduce bone resorp-
and is usually caused by clindamycin, ampicillin or ce-
tion such as bisphosphonates (100). In this regard,
phalosporins, especially in hospitalized patients (104,
doxycycline was recently shown to reduce crestal
bone resorption following endodontic flap reflection
One of the most serious side-effects of the frequent,
indiscriminate use of antibiotics, not only for the indi-vidual patient but also from a global public health
7) What are the potential side-
perspective, is the development of resistant bacterial
effects of using antibiotics?
strains (106–109). As was noted before, the percen-tage of b-lactamase-positive bacteria tends to increase
As clinicians make decisions on whether or not to pre-
in endodontic infections in patients with prior use of
scribe antibiotics in conjunction with endodontic
b-lactam antibiotics (49). Another group of micro-
treatment, it is important to be cognizant of the risks
organisms that are becoming among the most serious
and side-effects of antibiotics. The use of antibiotics
drug-resistant bacteria are enterococci (110). Enter-
is not different from any other medications in that
ococci, particularly E. faecalis and E. faecium, were
the benefits of using them must outweigh the risks
shown to be the most prevalent among the microflora
involved, from the perspectives of both the direct
of root canals in failing endodontic cases in a number
Fig. 1. General recommendations for use of antibiotics in conjunction with endodontic therapy.
of studies (111–114). Recently, it was also shown that
agnosis and inclusion criteria failed to corroborate
these two microorganisms, isolated from root canal
specimens of 29 endodontic cases following root ca-
Systemic antibiotic administration should be con-
nal instrumentation and medication, had multidrug
sidered if there is a spreading infection that signals
resistance properties. They were resistant to ben-
failure of local host responses in abating the advanc-
zylpenicillin, ampicillin, clindamycin, metronidazole
ing bacterial irritants, or if the patient’s medical his-
and tetracycline but were only sensitive to erythro-
tory includes conditions or diseases known to reduce
mycin and vancomycin (115). This further under-
the host defense mechanisms or expose the patient to
scores the importance of limiting the use of antibiotic
higher systemic risks. The effectiveness of antibiotic
to cases where they are specifically indicated.
administration in these conditions is not predictable,nor is the choice of which antibiotic to use estab-
Conclusions and general
lished, due to the polymicrobial nature of endodontic
recommendations
infections, and the fact that systemic antibiotics maynot reach the source of bacterial proliferation, such as
The current evidence indicates that local root canal
the necrotic pulp, in sufficient concentrations. There-
instrumentation procedures, combined with analgesic
fore, the emphasis should always be on instituting lo-
medications are sufficient for management of the vast
cal debridement and antimicrobial measures. The pa-
majority of symptomatic endodontic cases. When di-
tient must be followed closely until the condition re-
agnosing a case with odontogenic infection, it is im-
solves. If the condition does not resolve, then changes
portant that the clinician make a distinction between
in antibiotic therapy, culture and sensitivity testing or
localized infections, which may include cases with
prompt referral should be instituted.
periradicular radiolucencies, pain and localized swell-
The nonantibacterial beneficial properties of certain
ings, and those with spreading systemic infections.
antibiotics such as tetracyclines and the newer macro-
Antibiotic treatment is generally not recommended
lides should be further studied, particularly if subanti-
for healthy patients with localized endodontic infec-
microbial doses can be used locally, thereby reducing
tions. While one study showed advantages of the use
the danger of development of resistant bacterial
of certain antibiotics in enhancing endodontic pain
resolution, more recent studies with well-defined di-
In conclusion, the elimination of the local microbial
factors remains the main treatment focus in the symp-
16. Akimoto Y et al. Ampicillin concentrations in human den-
tal granuloma after a single oral administration of talampic-
tomatic endodontic patient. Figure 1 proposes a rec-
illin. Antimicrob Agents Chemother 1988: 32: 566–567.
ommendation for the use of antibiotics in conjunc-
17. Uda A et al. Josamycin concentrations in human dental
granuloma after a single oral administration of josamycin. Gen Pharmac 1989: 20: 823–825.
18. Tuominen RKR, Lehtinen J. Peltola et al. Penetration of
References
erythromycin into periapical lesions after repeated doses oferythromycin acistrate and erythromycin stearate: a pilot
1. Dorn SO, Moodnik RM, Feldman MJ, Borden BG. Treat-
study. Oral Surg Oral Med Oral Pathol 1991: 71: 684–688.
ment of the endodontic emergency: a report based on a
19. Allard U. Antibiotics in exudate from periapical lesions in
questionnaire ª part I. J Endod 1977: 3: 94–100.
dogs. Endod Dent Traumatol 1989: 5: 287–291.
2. Dorn SO, Moodnik RM, Feldman MJ, Borden BG. Treat-
20. Oguntebi BR, DeSchepper EJ, Taylor TS, White CL, Pink
ment of the endodontic emergency: a report based on a
FE. Postoperative pain incidence related to the type of
questionnaire ª part II. J Endod 1977: 3: 153–156.
emergency treatment of symptomatic pulpitis. Oral Surg
3. Gatewood RS, Himel VT, Dorn SO. Treatment of the en-
Oral Med Oral Pathol 1992: 73: 479–483.
dodontic emergency: a decade later. J Endod 1990: 16:
21. Lepinski AM, Haegreaves KM, Goodis HE, Bowles WR.
Bradykinin levels in dental pulp by microdialysis. J Endod
4. Yingling NM, Byrne BE, Hartwell GR. Antibiotic use by
2000: 26: 744–747.
members of the American Association of Endodontists in
22. Cohen JS, Reader A, Fertel R, Beck M, Meyers WJ. A
the year.: report of a national survey. J Endod 2000: 28:
radioimmunoassay determination of the concentrations of
prostaglandins E2 and F2a in painful and asymptomatic
5. Whitten BH, Gardiner DL, Jeansonne BG, Lemon RR.
human dental pulps. J Endod 1985: 11: 330–335.
Current trends in endodontic treatment. report of a na-
23. Hahn CL, Falkler WA Jr, Minah GE. Microbiological
tional survey. J Am Dent Assoc 1996: 127: 1333–1341.
studies of carious dentine from human teeth with irrevers-
6. Eleazer PD. Pharmacology for endodontics. In: Ingle J,
ible pulpitis. Arch Oral Biol 1991: 36: 147–153.
Bakland L, eds. Endodontics. Hamilton, Ontario: BC
24. Hahn CL, Falkler WA Jr. Antibodies in normal and dis-
eased pulps reactive with microorganisms isolated from
7. Hargreaves KM, Hutter JW. Endodontic pharmacology.
deep caries. J Endod 1992: 18: 28–31.
In: Cohen S, Burns CB, eds. Pathways of the pulp, St.
25. Hahn CL. Falkler WA Jr, Minah GE. Correlation between
thermal sensitivity and microorganisms isolated from deep
8. Dahlen G. Microbiology and treatment of dental abscesses
carious dentin. J Endod 1993: 19: 26–30.
and periodontal-endodontic lesions. Periodontology 2000,
26. Nagle D, Reader A, Beck M, Weaver J. Effect of systemic
2002: 28: 206–239.
penicillin on pain in untreated irreversible pulpitis. Oral
9. Baumgartner CJL, Bakland, Sugita EI. Microbiology of
Surg Oral Med Oral Pathol Oral Radiol Endod 2000: 90:
endodontics and asepsis in endodontic practice. In: Ingle
J, Bakland L, eds. Endodontics. Hamilton, Ontario: BC
27. Imura N, Zuolo ML. Factors associated with endodontic
flare-ups: a prospective study. Int Endod J 1995: 28: 261–
10. Siqueira JF. Jr. Endodontic infections. Concepts, para-
digms, and perspectives. Oral Surg Oral Med Oral Pathol
28. Torabinejad MJD et al. Factors associated with endodontic
Oral Radiol Endod 2002: 94: 281–293.
interappointment emergencies of teeth with necrotic
11. Akimoto Y, Komiya M, Kaneko K, Fujii A, Tamura T.
pulps. J Endod 1988: 14: 261–266.
Ampicillin concentrations in human serum, gingiva, man-
29. Walton R, Fouad A. Endodontic interappointment flare-
dibular bone, dental follicle, and dental pulp following a
ups. a prospective study of incidence and related factors. J
single oral administration of bacampicillin. J Oral Maxillo-Endod 1992: 18: 172–177. fac Surg 1986: 44: 107–112.
30. Fouad AF, Rivera EM, Walton RE. Penicillin as a supple-
12. Wang MM, Hoover J, Ludington JR, Jr, White RR. Pres-
ment in resolving the localized acute apical abscess. Oral
ence of systemic ampicillin in pulp-extirpated root canals. Surg Oral Med Oral Pathol Oral Radiol Endod 1996: 81: J Endod 1988: 14: 502–507.
13. Bystedt H, Dornbusch K, Nord CE. Concentrations of az-
31. Henry M, Reader A, Beck M. Effect of penicillin on post-
idocillin, erythromycin, doxycycline and clindamycin in
operative endodontic pain and swelling in symptomatic ne-
human mandibular bone. Int J Oral Surg 1978: 7: 442–
crotic teeth. J Endod 2001: 27: 117–123.
32. Torabinejad MSO et al. Effectiveness of various medi-
14. Akimoto Y, Kaneko K, Fujii A, Yamamoto H. Ampicillin
cations on postoperative pain following root canal obtu-
concentrations in human radicular granuloma following a
ration. J Endod 1994: 20: 427–431.
single oral dose of bacampicillin. J Oral Maxillofac Surg
33. Torabinejad M et al. Effectiveness of various medications
1992: 50: 11–13.
on postoperative pain following complete instrumentation.
15. Akimoto YY, Mochizuki A, Uda H et al. Ampicillin con-
J Endod 1994: 20: 345–354.
centrations in radicular cysts following a single oral admin-
34. Rosenberg PA, Babick PJ, Schertzer L, Leung A. The ef-
istration of bacampicillin. Gen Pharmac 1993: 24: 895–
fect of occlusal reduction on pain after endodontic instru-
mentation. J Endod 1998: 24: 492–496.
35. Schuman NJ, Owens BM. Ludwig’s angina following den-
51. Sundqvist G, Reuterving CO. Isolation of Actinomyces is-
tal treatment of a five-year-old male patient: report of a
raelii from periapical lesion. J Endod 1980: 6: 602–606.
case. J Clin Pediatr Dent 1992: 16: 263–265.
52. Happonen RP, Viander M, Pelliniemi LJ. Immunoelectron
36. Stoykewych AA, Beecroft WA, Cogan AG. Fatal necrotiz-
microscopic study of Actinomyces colony in odontogenic
ing fasciitis of dental origin. J Can Dent Assoc 1992: 58:
periapical infection. Int J Oral Surg 1984: 13: 539–544.
53. Happonen RP, Soderling E, Viander M, Linko-Kettunen
37. Garatea-Crelgo J, Gay-Escoda C. Mediastinitis from
L, Pelliniemi LJ. Immunocytochemical demonstration of
odontogenic infection. Report of three cases and review of
Actinomyces species and Arachnia propionica in periapical
the literature. Int J Oral Maxillofac Surg 1991: 20: 65–
infections. J Oral Pathol 1985: 14: 405–413.
54. Happonen RP. Periapical actinomycosis. a follow-up study
38. Bonapart IE, Stevens HP, Kerver AJ, Rietveld AP. Rare
of 16 surgically treated cases. Endod Dent Traumatol
complications of an odontogenic abscess: mediastinitis,
1986: 2: 205–209.
thoracic empyema and cardiac tamponade. J Oral Maxillo-
55. Happonen RP. Immunocytochemical diagnosis of cervico-
fac Surg 1995: 53: 610–613.
facial actinomycosis with special emphasis on periapical in-
39. Heimdahl A, von Konow L, Satoh T, Nord CE. Clinical
flammatory lesions. Proc Finn Dent Soc 1986: 82 (Suppl
appearance of orofacial infections of odontogenic origin in
relation to microbiological findings. J Clin Microbiol 1985:
56. Barnard D, Davies J, Figdor D. Susceptibility of Acti-
22: 299–302.
nomyces israelii to antibiotics, sodium hypochlorite and
40. van Winkelhoff AJ, VanDenBroucke-Grauls CM. Microbio-
calcium hydroxide. Int Endod J 1996: 29: 320–326.
logical sampling and sensitivity testing. In: Newman MG,
57. Ranta HM, Haapasalo K. Ranta et al. Bacteriology of
Van Winkelhoff AJ, eds. Antibiotic and antimicrobial use in
odontogenic apical periodontitis and effect of penicillin
dental practice Chicago: Quintessence, 2001: 21–29.
treatment. Scand J Infect Dis 1988: 20: 187–192.
41. Goldman M, Pearson AH. A clinical study of the use of
58. Gilmore WC, Jacobus NV, Gorbach SL, Doku HC, Tally
antibiotic sensitivity testing in endodontics. Oral Surg
FP. A prospective double-blind evaluation of penicillin ver-
Oral Med Oral Pathol 1962: 15: 1250–1258.
sus clindamycin in the treatment of odontogenic infec-
42. Lewis MA. MacFarlane TW, McGowan DA. Antibiotic
tions. J Oral Maxillofac Surg 1988: 46: 1065–1070.
susceptibilities of bacteria isolated from acute dentoalve-
59. Mangundjaja S, Hardjawinata K. Clindamycin versus ampi-
olar abscesses. J Antimicrob Chemother 1989: 23: 69–77.
cillin in the treatment of odontogenic infections. Clin Ther
43. Lana MAAP et al. Microorganisms isolated from root ca-
1990: 12: 242–249.
nals presenting necrotic pulp and their drug susceptibility
60. Schuen NJ, Panzer JD, Atkinson WH. A comparison of
in vitro. Oral Microbiol Immunol 2001: 16: 100–105.
clindamycin and penicillin V in the treatment of oral infec-
44. Kuriyama T, Karasawa T, Nakagawa K, Yamamoto E, Nak-
tions. J Oral Surg 1974: 32: 503–505.
amura S. Incidence of b-lactamase production and anti-
61. Lewis MA, Carmichael F, MacFarlane TW, Milligan SG. A
microbial susceptibility of anaerobic gram-negative rods
randomised trial of co-amoxiclav (Augmentin) versus peni-
isolated from pus specimens of orofacial odontogenic in-
cillin V in the treatment of acute dentoalveolar abscess.
fections. Oral Microbiol Immunol 2001: 16: 10–15. Br Dent J 1993: 175: 169–174.
45. Ernest MA, Conte MV, Keudell KC. Antibiotic sensitivity
62. Fazakerley MW, McGowan P, Hardy P, Martin MV. A
patterns of facultative and obligate anaerobic bacteria from
pulp canals. J Endod 1977: 3: 106–109.
phenoxymethylpenicillin in the treatment of acute dento-
46. Le Goff AL, Bunetel C, Mouton, M. Bonnaure-Mallet.
alveolar infection. Br Dent J 1993: 174: 359–363.
Evaluation of root canal bacteria and their antimicrobial
63. Quirynen M, Teughels W, De Soete M, van Steenberghe
susceptibility in teeth with necrotic pulp. Oral Microbiol
D. Topical antiseptics and antibiotics in the initial therapy
Immunol 1997: 12: 318–322.
of chronic adult periodontitis: microbiological aspects.
47. Kuriyama T, Karasawa T, Nakagawa K, Yamamoto E, Nak-
Periodontology 2000, 2002: 28: 72–90.
amura S. Bacteriology and antimicrobial susceptibility of
64. Rams TE, Slots J. Local delivery of antimicrobial agents in
gram-positive cocci isolated from pus specimens of oro-
the periodontal pocket. Periodontology 2000, 1996: 10:
facial odontogenic infections. Oral Microbiol Immunol
2002: 17: 132–135.
65. Walker C, Karpinia K. Rationale for use of antibiotics in
48. Kuriyama T et al. Bacteriologic features and antimicrobial
periodontitis. J Periodontol 2002: 73: 1188–1196.
susceptibility in isolates from orofacial odontogenic infec-
66. Abbott PV, Hume WR, Pearman JW. Antibiotics and en-
tions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
dodontics. Aust Dent J 1990: 35: 50–60.
2000: 90: 600–608.
67. Haznedaroglu F, Ersev H. Tetracycline HCl solution as a
49. Kuriyama T et al. Past administration of b-lactam anti-
root canal irrigant. J Endod 2001: 27: 738–740.
biotics and increase in the emergence of b-lactamase-pro-
68. Sanz M, Herrera D. Individual drugs. In: Newman MG,
ducing bacteria in patients with orofacial odontogenic in-
Van Winkelhoff AJ, eds. Antibiotic and antimicrobial use
fections. Oral Surg Oral Med Oral Pathol Oral Radiolin dental practice. Chicago: Quintessence, 2001: 33–52. Endod 2000: 89: 186–192.
69. Weine F. Endodontic therapy, 5th edn. St. Louis: Mosby,
50. Kuriyama T, Karasawa T, Nakagawa K, Nakamura S, Yama-
moto E. Antimicrobial susceptibility of major pathogens of
70. Grossman LI. Treatment of pulpless teeth with a concen-
orofacial odontogenic infections to 11 b-lactam anti-
trated sulfonamid solution. J Am Dent Assoc 1945: 32:
biotics. Oral Microbiol Immunol 2002: 17: 285–289.
71. Grossman LI. Polyantibiotic treatment of pulpless teeth. J
Erythromycin modulates eosinophil chemotactic cytokine
Am Dent Assoc 1951: 43: 265–278.
production by human lung fibroblasts in vitro. Antimicrob
72. Grossman LI. Evaluation of penicillemia after medication
Agents Chemother 2001: 45: 401–406.
of root canals with a polyantibiotic. J Dent Res 1967: 46:
92. Kurdowska A, Noble JM, Griffith DE. The effect of az-
ithromycin and clarithromycin on ex vivo interleukin-8
73. Grossman LI. Sterilization of infected root canals. J Am
(IL-8) release from whole blood and IL-8 production by
Dent Assoc 1972: 85: 900–905.
human alveolar macrophages. J Antimicrob Chemother
74. Nicholls E. Endodontics, 3rd edn. Bristol: Wright, 1984:
2001: 47: 867–870.
93. Moore PA. Dental therapeutic indications for the newer
75. Abbott PV, Heithersay GS, Hume WR. Release and dif-
long-acting macrolide antibiotics. J Am Dent Assoc 1999:
fusion through human tooth roots in vitro of cortico-
130: 1341–1343.
steroid and tetracycline trace molecules from Ledermix
94. Morse DRML et al. Infectious flare-ups and serious seque-
paste. Endod Dent Traumatol 1988: 4: 55–62.
lae following endodontic treatment: a prospective ran-
76. Abbott PV, Hume WR, Heithersay GS. Effects of combin-
domized trial on efficacy of antibiotic prophylaxis in cases
ing Ledermix and calcium hydroxide pastes on the dif-
of asymptomatic pulpal-periapical lesions. Oral Surg Oral
fusion of corticosteroid and tetracycline through human
Med Oral Pathol 1987: 64: 96–109.
tooth roots in vitro. Endod Dent Traumatol 1989: 5: 188–
95. Golub LMHM et al. Tetracyclines inhibit connective tissue
breakdown by multiple non-antimicrobial mechanisms.
77. Shovelton DS, Friend LA, Kirk EE, Rowe AH. The effi-
Adv Dent Res 1998: 12: 12–26.
cacy of pulp capping materials. A comparative trial. Br
96. Golub LM et al. Adjunctive treatment with subantimicrob-
Dent J 1971: 130: 385–391.
ial doses of doxycycline: effects on gingival fluid collagen-
78. Barthel CR, Rosenkranz B, Leuenberg A, Roulet JF. Pulp
ase activity and attachment loss in adult periodontitis. J
capping of carious exposures: treatment outcome after 5
Clin Periodontol 2001: 28: 146–156.
and 10 years: a retrospective study. J Endod 2000: 26:
97. Ryan ME, Ashley RA. How do tetracyclines work? AdvDent Res 1998: 12: 149–151.
79. Trope M. Relationship of intracanal medicaments to endo-
98. Fouad A. Molecular mediators of pulpal inflammation. In:
dontic flare-ups. Endod Dent Traumatol 1990: 6: 226–
Hargreaves KM, Goodis HE, eds. Seltzer and Bender’s den-tal pulp, Chicago: Quintessence, 2002: 247–279.
80. Molander A, Reit C, Dahlen G. Microbiological evaluation
99. Gusman H, Santana RB, Zehnder M. Matrix metallopro-
of clindamycin as a root canal dressing in teeth with apical
teinase levels and gelatinolytic activity in clinically healthy
periodontitis. Int Endod J 1990: 23: 113–118.
and inflamed human dental pulps. Eur J Oral Sci 2002:
81. Gilad JZ, Teles R, Goodson M, White RR, Stashenko P. 110: 353–357.
Development of a clindamycin-impregnated fiber as an in-
100. Llavaneras ANS et al. A combination of a chemically modi-
tracanal medication in endodontic therapy. J Endod 1999:
fied doxycycline and a bisphosphonate synergistically in-
25: 722–727.
hibits endotoxin-induced periodontal breakdown in rats. J
82. Miyatake HF et al. Erythromycin reduces the severity of
Periodontol 2001: 72: 1069–1077.
bronchial hyperresponsiveness in asthma. Chest 1991: 99:
101. Cummings GR, Torabinejad M. Effect of systemic doxycy-
cline on alveolar bone loss after periradicular surgery. J En-
83. Itkin IH, Menzel ML. The use of macrolide antibiotic sub-
dod 2000: 26: 325–327.
stances in the treatment of asthma. J Allergy 1970: 45:
102. Cunha BA. Antibiotic side effects. Med Clin North Am
2001: 85: 149–185.
84. Wolter JS et al. Effect of long term treatment with azithro-
103. Baker KA, Fotos PG. The management of odontogenic
mycin on disease parameters in cystic fibrosis: a random-
infections. A rationale for appropriate chemotherapy. Dent
ised trial. Thorax 2002: 57: 212–216. Clin North Am 1994: 38: 689–706.
85. Koyama H, Geddes DM. Erythromycin and diffuse pan-
104. Sensakovic JW, Smith LG. Oral antibiotic treatment of in-
bronchiolitis. Thorax 1997: 52: 915–918.
fectious diseases. Med Clin North Am 2001: 85: 115–123.
86. Scaglione F, Rossoni G. Comparative anti-inflammatory
105. Sandor GK, Low DE, Judd PL, Davidson RJ. Anti-
effects of roxithromycin, azithromycin and clarithromycin.
microbial treatment options in the management of odon-
J Antimicrob Chemother 1998: 41: 47–50.
togenic infections. J Can Dent Assoc 1998: 64: 508–514.
87. Ianaro AA et al. Anti-inflammatory activity of macrolide
106. Handal T, Olsen I. Antimicrobial resistance with focus on
antibiotics. J Pharmacol Exp Ther 2000: 292: 156–163.
oral b-lactamases. Eur J Oral Sci 2000: 108: 163–174.
88. Xu GJ et al. Effect of macrolide antibiotics on macrophage
107. Jenkinson HF. Ins and outs of antimicrobial resistance: era
functions. Microbiol Immunol 1996: 40: 473–479.
of the drug pumps. J Dent Res 1996: 75: 736–742.
89. Anderson R, Theron AJ, Feldman C. Membrane-stabil-
108. Harrison JW, Svec TA. The beginning of the end of the
izing, anti–inflammatory interactions of macrolides with
antibiotic era? Part I. The problem: abuse of the ‘miracle
human neutrophils. Inflammation 1996: 20: 693–705.
drugs’. Quintessence Int 1998: 29: 151–162.
90. Shimane T, Asano K, Suzuki M, Hisamitsu T, Suzaki H.
109. Harrison JW, Svec TA. The beginning of the end of the
Influence of a macrolide antibiotic, roxithromycin, on
antibiotic era? Part II. Proposed solutions to antibiotic
mast cell growth and activation in vitro. Med Inflamm
abuse. Quintessence Int 1998: 29: 223–229.
2001: 10: 323–332.
110. Kaye KS, Fraimow HS, Abrutyn E. Pathogens resistant to
91. Sato E, Nelson DK, Koyama S, Hoyt JC, Robbins RA.
antimicrobial agents. Epidemiology, molecular mechan-
isms, and clinical management. Infect Dis Clin North Am
ic analysis of teeth with failed endodontic treatment and the
2000: 14: 293–319.
outcome of conservative re-treatment. Oral Surg Oral Med
111. Hancock HH. 3rd, Sigurdsson A, Trope M, Moiseiwitsch
Oral Pathol Oral Radiol Endod 1998: 85: 86–93.
J. Bacteria isolated after unsuccessful endodontic treatment
114. Molander A, Reit C, Dahlen G, Kvist T. Microbiological
in a North American population. Oral Surg Oral Med Oral
status of root-filled teeth with apical periodontitis. Int En-Pathol Oral Radiol Endod 2001: 91: 579–586. dod J 1998: 31: 1–7.
112. Peciuliene V, Balciuniene I, Eriksen HM, Haapasalo M. Iso-
115. Dahlen G, Samuelsson W, Molander A, Reit C. Identifi-
lation of Enterococcus faecalis in previously root-filled canals
cation and antimicrobial susceptibility of enterococci iso-
in a Lithuanian population. J Endod 2000: 26: 593–595.
lated from the root canal. Oral Microbiol Immunol 2000:
113. Sundqvist G, Figdor D, Persson S, Sjogren U. Microbiolog-
15: 309–312.
MARCH 11, 2008 MINUTES OF THE BEAVER CITY COUNCIL:The Beaver City Council met in regular session on the 11 daycommenced at 4:00 p.m. The following Council Members were present: Mayor Leonard Foster,City Council Members; Kari Draper, Connie Fails, Craig Wright, Gordon Roberts and Chris Smith. Also, present at the meeting: City Recorder Hal Lessing and City Manager Steve Atkin. Mayor Foster conduc
ALKOHOLFREIE GETRÄNKE Allegra - Mineralwasser ohne Kohlensäure Passuger - Mineralwasser mit Kohlensäure Henniez - Mineralwasser mit wenig Kohlensäure Légère Knutwiler - Mineralwasser MIT oder OHNE Kohlensäure Zitrone, Mandarin, Heidelbeere, Grapefruit, Bitterorange, Himbeere Ramseier Süssmost - Apfelsaft Schweppes - Bitter Lemon, Tonic Water oder Ginger Ale Tomaten, Orangen, Grapef
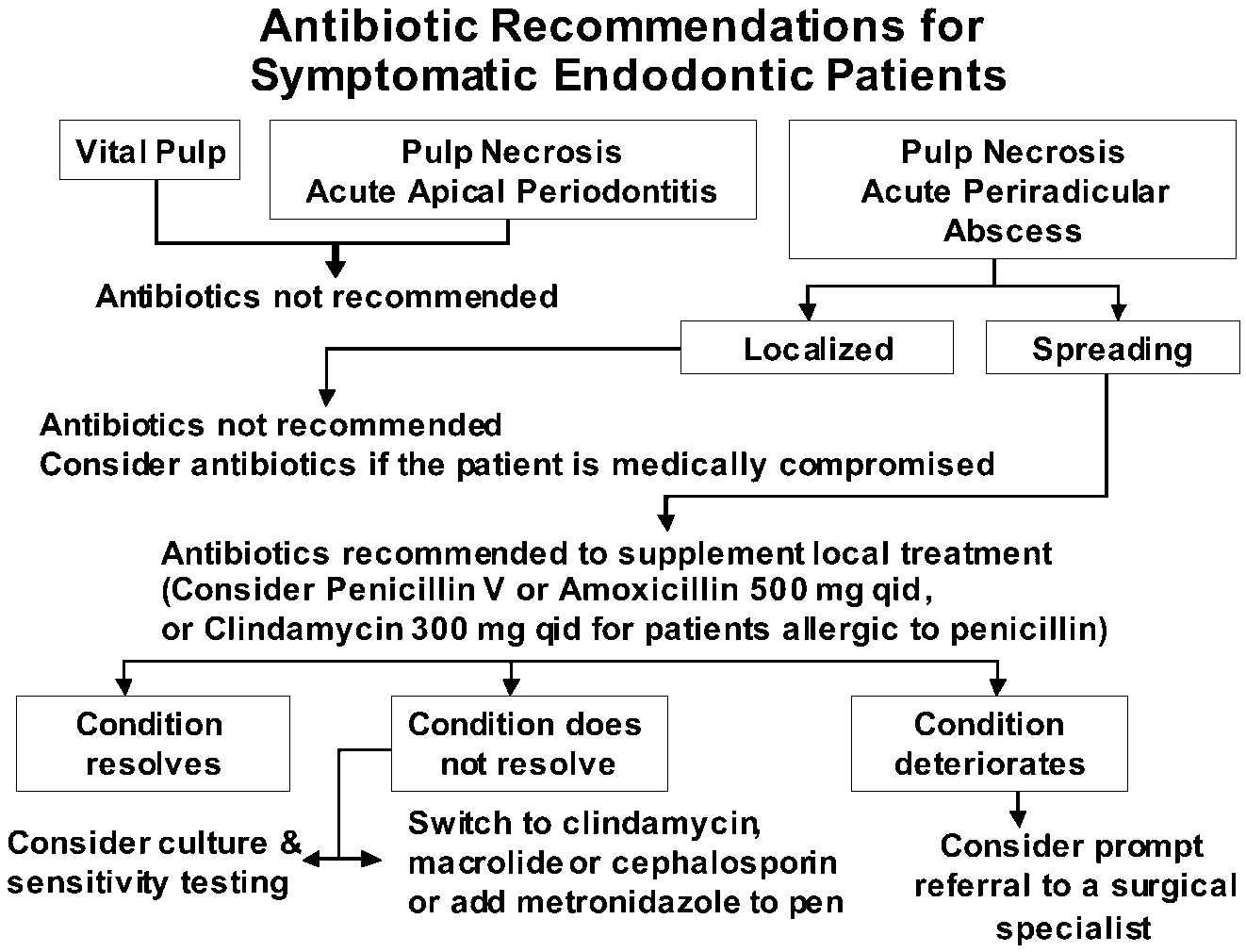 Fig. 1. General recommendations for
Fig. 1. General recommendations for