The osmolyte xylitol reduces the salt concentration of airway surface liquid and may enhance bacterial killing Joseph Zabner*†, Michael P. Seiler*, Janice L. Launspach*, Philip H. Karp*, William R. Kearney‡, Dwight C. Look§, Jeffrey J. Smith¶, and Michael J. Welsh*ʈ**
ʈHoward Hughes Medical Institute, Departments of *Internal Medicine, ¶Pediatrics, and **Physiology and Biophysics, and ‡Nuclear Magnetic ResonanceFacility, University of Iowa College of Medicine, Iowa City, IA 52242; and §Department of Medicine, Washington University, St. Louis, MO 63110
Contributed by Michael J. Welsh, August 7, 2000
The thin layer of airway surface liquid (ASL) contains antimicrobial
an effect could be of value in preventing airway infections,
substances that kill the small numbers of bacteria that are con-
irrespective of the absolute salt concentration in ASL or of
stantly being deposited in the lungs. An increase in ASL salt
differences between CF and non-CF. We considered several
concentration inhibits the activity of airway antimicrobial factors
factors. First, the airway epithelium is water permeable (17). and may partially explain the pathogenesis of cystic fibrosis (CF).
Consistent with this finding, when large volumes of liquid are
We tested the hypothesis that an osmolyte with a low transepi-
placed on the apical surface, liquid absorption is isotonic (9, 15). thelial permeability may lower the ASL salt concentration, thereby
Thus, if water were simply added to the airway surface, electro-
enhancing innate immunity. We found that the five-carbon sugar
lyte concentrations would rapidly return to starting values. xylitol has a low transepithelial permeability, is poorly metabolized
However, if an osmolyte that has a low transepithelial perme-
by several bacteria, and can lower the ASL salt concentration in
ability were added to ASL, it might serve to lower the salt
both CF and non-CF airway epithelia in vitro. Furthermore, in a
concentration. Somewhat analogous to this effect, the relatively
double-blind, randomized, crossover study, xylitol sprayed for 4
impermeable osmolyte lactose allows the water-permeable
days into each nostril of normal volunteers significantly decreased
mammary gland duct epithelium to maintain the luminal NaCl
the number of nasal coagulase-negative Staphylococcus compared
concentration at 5–10 mM (18). Second, an osmolyte that is
with saline control. Xylitol may be of value in decreasing ASL salt
nonionic would be required, because it is ionic strength that
concentration and enhancing the innate antimicrobial defense at the airway surface.
inhibits antimicrobial activity, not osmolarity (19, 20). Third, the
osmolyte should not provide a ready carbon source for bacterial
A thin layer of liquid covering the airway surface (ASL) growth. Fourth, the osmolyte should be safe in humans. Fifth,
contains many antimicrobial substances, including ly-
because many endogenous antimicrobials kill very quickly, even
sozyme, lactoferrin, secretory leukoproteinase inhibitor, human
a transient decrease in ionic strength might be effective. Finally,
 defensins 1 and 2, secretory phospholipase A2, and the
a small reduction in the salt concentration, perhaps only 10 mM,
cathelicidin LL-37 (for reviews see refs. 1–4). These agents
might be beneficial because there is no unique relationship
acting alone and synergistically form part of the local pulmonary
between antimicrobial activity and ionic strength; the lower the
host defense system, killing the small numbers of bacteria that
ionic strength, the greater the bacterial killing (20–22).
are constantly being deposited on the airway surface. The
A promising osmolyte for lowering ASL ionic strength is the
antibacterial activity of most of these agents is salt-sensitive; an
five-carbon sugar, xylitol, which is poorly metabolized by some
increase in salt concentration inhibits the activity of individual
bacteria (23). Interestingly, when incorporated into chewing
factors and attenuates synergy between agents.
gum, xylitol is reported to prevent dental caries (24). Moreover,
We recently proposed that disruption of this innate defense
in chewing gum, lozenges, or syrup, xylitol decreases the inci-
system causes, in part, the well-known propensity of cystic
dence of acute otitis media by 20–40% (25). Therefore, we tested
fibrosis (CF) airways for bacterial infection (5). CF lung disease
the hypothesis that xylitol applied to the apical surface of human
is initially characterized by infection with a variety of bacteria,
airway epithelia would lower the ASL salt concentration. We
and as the disease progresses Staphylococcus aureus and Pseudo-
also examined the effect of xylitol on bacteria in vitro and in vivo. monas aeruginosa predominate (5, 6). We hypothesized that the
loss of cystic fibrosis transmembrane conductance ClϪ channels
leads to a higher ASL salt concentration, which reduces antimi-
Materials and Methods
crobial potency and thereby impairs the innate immune system
Human Airway Epithelia. Airway epithelial cells were isolated from
(7, 8). Several studies using in vitro model systems of the human
tracheal and bronchial tissue, grown on semipermeable mem-
airway have reported that salt concentrations are lower in ASL
branes at the air-liquid interface, and studied at least 14 days
than in serum and are elevated in CF (8–11). However, the
after seeding when they had differentiated and developed a
applicability of these observations to the in vivo human airway
ciliated apical surface (26, 27). Transepithelial resistance was
has not been established with certainty. Some in vivo studies have
588 Ϯ 33 ⍀⅐cm2 (n ϭ 9) for non-CF and 493 Ϯ 24 ⍀⅐cm2 (n ϭ
reported low NaCl concentrations in non-CF and higher values
in CF ASL (12), whereas other reports have concluded that the
ASL NaCl is similar to that of serum in both non-CF and CF (13,
14). The difficulty in measuring ASL electrolyte concentrations
is due to its tiny volume (9, 15), to liquid application to the airway
Abbreviations: ASL, airway surface liquid; CF, cystic fibrosis; cfu, colony-forming units.
surface followed by measurements before a steady state is
†To whom reprint requests should be addressed at: University of Iowa College of Medicine,
achieved (15), and to artifacts associated with the use of filter
500 Eckstein Medical Research Building, Iowa City, IA 52242. E-mail: [email protected].
We hypothesized that lowering the ASL NaCl concentration
The publication costs of this article were defrayed in part by page charge payment. Thisarticle must therefore be hereby marked “advertisement” in accordance with 18 U.S.C.
could increase the activity of endogenous antimicrobials. Such
§1734 solely to indicate this fact. 11614 –11619 ͉ PNAS ͉ October 10, 2000 ͉ vol. 97 ͉ no. 21 Measurement of Xylitol Fluxes. To the apical surface we applied 60
to 103) in the presence or absence of 100 mM xylitol and
l of a xylitol solution containing (in mM) 138 xylitol, 53 NaCl,
4 KCl, 29 NaHCO3, 1.2 CaCl2, 0.6 MgCl2, and 1 NaH2PO4. The
To test the effect of xylitol on the growth of normal nasal flora
osmolality of the submucosal solution was adjusted to equal that
in a carbon-starved medium, we obtained nasal swabs from three
of the mucosal solution with a vapor pressure osmometer
normal volunteers and inoculated the swabs into M9 medium
(Wescor, Logan, UT). To the apical and basolateral solutions we
alone, M9 with 100 mM xylitol, or LB medium. Bacteria were
added 1 ϫ 106 cpm͞ml of 3H2O. The apical solution also received
incubated at 37°C for 72 h, and the ODs were recorded.
1 ϫ 106 cpm͞ml of 14C-labeled xylitol (Moravek Biochemicals,
Brea, CA). After incubation at 37°C for 1–12 h, both solutions
Administration of Xylitol to the Nasal Mucosa. The study was
were collected and the volume and xylitol concentrations were
approved by the University of Iowa Institutional Review Board.
determined; the methods have been described (9).
Subjects were more than 18 years old and provided written
informed consent. Individuals were excluded from participation
Measurement of Liquid Absorption and Xylitol. Liquid absorption
if they had a seasonal allergic rhinitis or nasal polyps, or current
was measured using methods similar to those previously de-
treatment with any antibiotic, steroid, or topical intranasal
scribed (9). To the apical surface we applied 60 l of a saline
preparation. Twenty-one normal healthy subjects (10 male and
solution, a xylitol solution, or a mixture of the two. The saline
11 female, ages 20–52 years) participated.
solution contained (in mM) 138 NaCl, 4 KCl, 29 NaHCO3, 1.2
The design was a double-blind, randomized, cross-over study.
CaCl2, 0.6 MgCl2, and 1 NaH2PO4. The xylitol solution con-
Subjects were randomized to one of two groups: xylitol followed
tained (in mM) 244 xylitol, 4 KCl, 29 NaHCO3, 1.2 CaCl2, 0.6
by saline or saline followed by xylitol. A culture of both anterior
MgCl2, and 1 NaH2PO4. The osmolality of the submucosal
nares was obtained on day 0. Subjects then sprayed each nostril
solution was adjusted to equal that of the mucosal (300-310
with a prefilled syringe of solution four times per day for 4 days.
mOsm) solution. After incubation for 4 h, apical solutions were
On the morning of day 5, subjects sprayed the final application
collected under mineral oil, and the volume was measured as
into each nostril at breakfast time, then a nasal swab was
obtained 2 h later. No treatment was administered for the next
7 days. Then subjects repeated the protocol with the opposite
Measurement of ASL Cl؊ Concentration. The ASL ClϪ concentra-
solution. The saline solution was 0.9% NaCl in water (Baxter
tion was measured as described (9). To the apical surface we
Health Care, Mundelein, IL); the xylitol solution was 5% xylitol
applied 5 l of a saline solution or a xylitol solution. The xylitol
(304 mM) in water. The solutions (250 l) were nebulized by
solution contained (in mM) 290 xylitol, 1.2 CaCl2, and 0.6 MgCl2.
using an Accuspray syringe (Becton Dickinson Pharmaceutical
The saline solution contained (in mM) 145 NaCl, 1.2 CaCl2, and
Systems, Franklin Lakes, NJ). Xylitol and saline syringes were
0.6 MgCl2. To the basolateral medium (500 l) we added 2.5 ϫ
identical. The mass medium diameter of the particles was ϳ60
104 cpm of 3H2O and 36Cl. ASL ClϪ concentration and volume
m. It was impossible to disguise the sweet taste of the xylitol.
Fifteen of the 21 subjects were able to recognize the sweet taste
of the xylitol; the other six subjects could not distinguish between
Evaluation of the Effect of Xylitol on Bacterial Growth. Procedures
were approved by the Human Subjects Review Board of the
Cultures were obtained with sterile rayon swabs (Culturette
University of Iowa. Nasal lavage fluid was collected from normal
Collection and Transport System; Becton Dickinson Microbiol-
volunteers. A flexible catheter (18-gauge; Jelco, Tampa, FL) was
ogy Systems, Sparks, MD). A swab was rotated firmly five times
inserted into each nostril, and the area was flushed four times
in each nostril. Swabs were collected by the same individual
with 4 ml of sterile water. Cells were removed by centrifugation,
throughout the study. Swabs were directly inoculated into 1 ml
and the fluid was filtered with a sequential 0.8͞0.2 m Supor
of PBS and vortexed for 5 s, and 50 l was plated by using an
Acrodisc PF (Gelman). To study the effect of xylitol on bacterial
automated spiral plater (Spiral Biotech, Bethesda, MD) onto
killing by endogenous antimicrobial factors, we used a lumines-
sheep blood agar (Remel, Lenexa, KS), and mannitol salt agar
PHYSIOLOGY
cence assay of bacterial viability in which Escherichia coli
(Becton Dickinson, Sparks, MD). Plates were incubated at 37°C
expresses the genes from Photorhabdus luminescens (20). Bac-
for 24 h, and colonies of coagulase-negative Staphylococcus
teria (106) were incubated with 50 l of nasal lavage fluid in
colonies were identified and counted by using a Cling-On Grid
serial dilutions of 300 mM xylitol or 150 mM NaCl in a 96-well
(Spiral Biotech). Samples were routinely sent to the Clinical
plate. Luminescence was measured after incubation at 30°C
Microbiology Laboratory (University of Iowa Hospitals and
Clinics) to confirm the identity of the bacteria.
To test the effect of xylitol on the growth of bacteria in a
In a preliminary study in eight non-CF subjects, we found that
carbon-starved medium, we grew P. aeruginosa, S. aureus, and
the number of coagulase-negative Staphylococcus cultured from
coagulase-negative Staphylococcus overnight in LB medium.
the nasal epithelium remained relatively stable over 4 days. A
Bacteria were centrifuged; resuspended in M9 medium contain-
power analysis (28) suggested that 39 independent nostrils would
ing 100 mM of succinate, mannitol, or sucrose; and grown
be required to show a 50% difference in the reduction in
overnight at 37°C. The bacteria were centrifuged and resus-
coagulase-negative Staphylococcus between treatments (power
pended in M9 medium alone, M9 medium containing 100 mM
of 0.84 and an f value of 0.5, assuming that the nostrils are
xylitol, or 100 mM indicated metabolizable sugar as a positive
independent). In contrast to non-CF subjects, we found that the
control and studied in midlog phase. OD was measured after 0,
numbers of bacteria cultured from the CF nasal surface were
To test the antibiotic effect of xylitol, P. aeruginosa, S. aureus,
and coagulase-negative Staphylococcus were grown overnight in
LB medium, centrifuged, and resuspended in LB medium with
Xylitol Permeability of Airway Epithelia. To examine the effect of
and without 100 mM xylitol. As a positive control, antibiotics
xylitol on ASL, we used primary cultures of well-differentiated
with activity to each of the bacteria were added to the medium
airway epithelia (26, 27). Because airway epithelia are water
(40 g͞ml tobramycin or 40 g͞ml levofloxacin). To test the
permeable (17), lowering ASL salt concentration will require an
antibiotic effect of xylitol on lower concentrations of coagulase-
osmolyte with a relatively low transepithelial permeability. We
negative Staphylococcus saprophyticus (ATCC 15305) over
tested the xylitol permeability by applying it to the apical surface
longer periods of time, we incubated log dilutions of bacteria (108
and measuring its disappearance over time. The amount of
PNAS ͉ October 10, 2000 ͉ vol. 97 ͉ no. 21 ͉ 11615
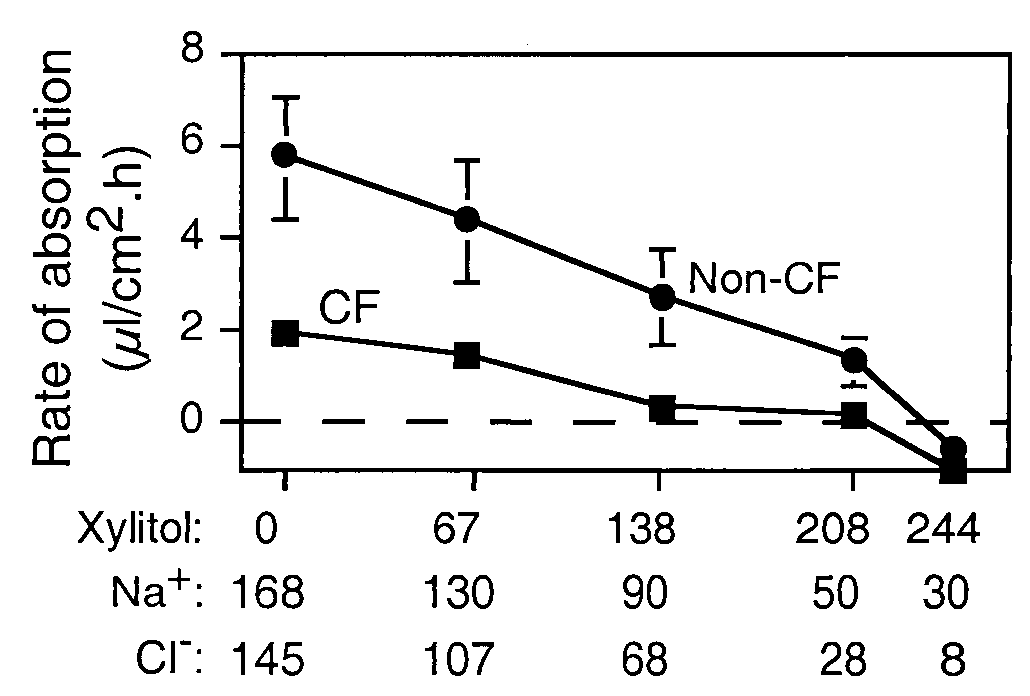
Effect of apical xylitol on the rate of liquid absorption by non-CF and
CF epithelia. Sixty microliters of saline solution, xylitol solution, or indicatedmixtures of the two was applied to the apical solution. Four hours later thesolution was removed to measure the rate of liquid absorption. A shortincubation period was chosen to avoid secondary changes in the epitheliumdue to the large volume of apical liquid. Data are mean Ϯ SEM (n ϭ 15) fromthree different experiments. Some SEM bars are hidden by symbols.
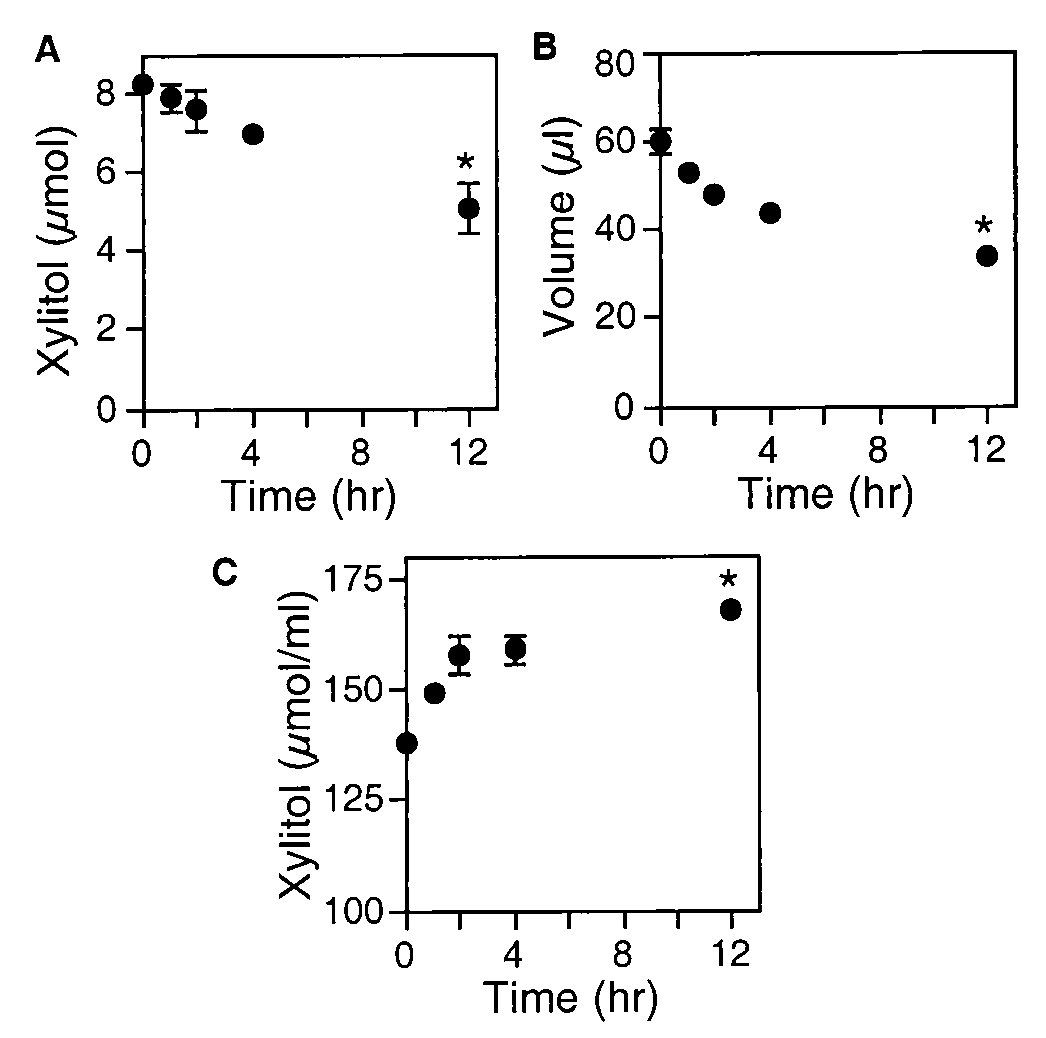
Apical xylitol and volume after the addition of xylitol to the apical
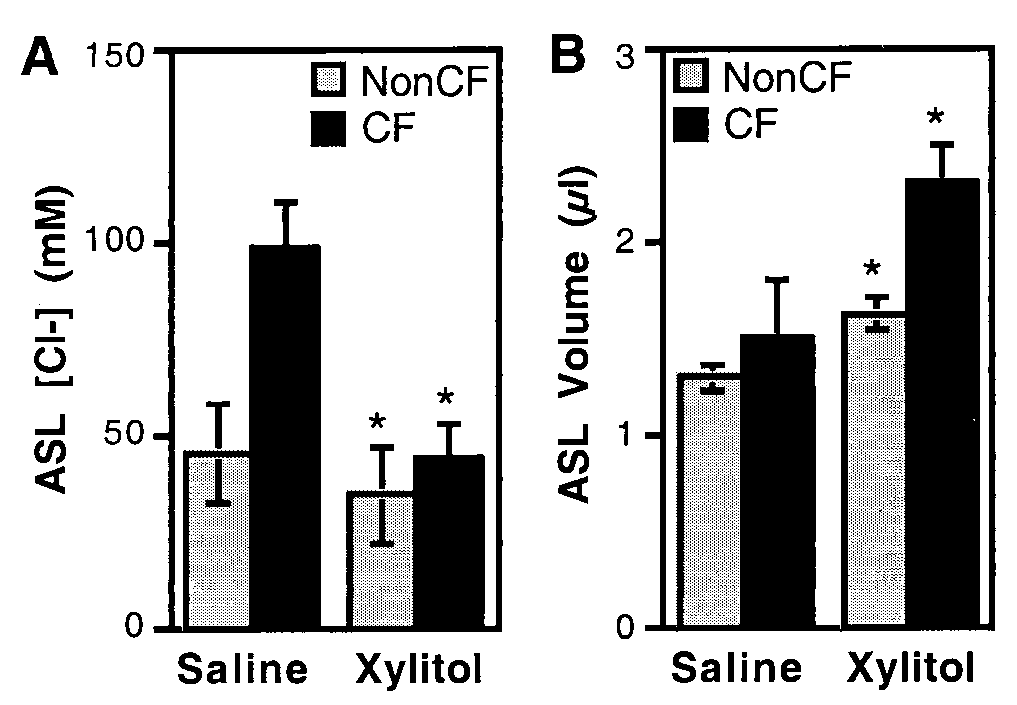
after the addition of saline (Fig. 3A). This value is approximately
surface of non-CF airway epithelia. Xylitol (138 mM in 60 l) was added to the
double that in non-CF epithelia and is consistent with our earlier
apical surface of differentiated airway epithelia at time 0. Then, at the times
measurements (9). However, with xylitol application, the ClϪ
indicated, the apical liquid was removed and the quantity of xylitol (A), the
concentration fell to values observed in non-CF epithelia. Xylitol
liquid volume (B), and the xylitol concentration (C) were determined. Data are
also increased the estimated ASL volume in both non-CF and CF
mean Ϯ SEM (n ϭ 6). Some SEM bars are hidden by symbols. The asterisk
epithelia (Fig. 3B). Thus, adding xylitol to the CF epithelial
indicates P Ͻ 0.01 compared with time 0.
surface allowed a reduction in ClϪ concentration that was likely
due to a combination of active transepithelial salt transport, ASL
xylitol progressively decreased; after 12 h, 40% of the applied
dilution, and the osmotic pressure generated by xylitol.
sugar had diffused to the basolateral surface (Fig. 1). Because
the volume decreased with time, the xylitol concentration in-
Xylitol Does Not Affect Bacterial Growth and Does Not Interfere with
creased. We obtained similar results when we measured the
Killing by Endogenous Antimicrobial Factors. Earlier data showed
concentration of xylitol by NMR (not shown). Thus the xylitol
that increased ionic strength, not increased osmolarity, inhibited
permeability was not high, and the increase in concentration
bacterial killing by endogenous airway antimicrobial factors (20).
suggested that xylitol could temporarily hold liquid on the apical
To test the effect of xylitol, we collected nasal lavage fluid, which
contains multiple antimicrobial factors, and examined killing of
To test this hypothesis directly, we asked whether xylitol
E. coli with a luminescence assay. Fig. 4 shows that nasal lavage
reduces the rate of liquid absorption. We applied 60 l of a saline
solution, a xylitol solution, or a mixture of the two to the apical
surface. The apical solution always had the same osmolarity as
the basolateral solution; thus as the xylitol concentration in-
creased, the NaCl concentration decreased. Four hours later, we
removed the liquid and determined the rate of liquid absorption.
Fig. 2 shows that during a 4-h incubation with apical saline, both
non-CF and CF epithelia absorbed liquid, and consistent with
our previous report the rate of liquid absorption was greater in
non-CF than in CF epithelia (9). In both non-CF and CF
epithelia, increasing the xylitol concentration reduced the rate of
liquid absorption (Fig. 2). Like the data in Fig. 1, these results
indicate that xylitol is relatively nonpermeable because it re-
duced the absorption rate and held liquid on the apical surface. Xylitol Added to the Apical Surface Decreases ASL Cl؊ Concentration in CF Epithelia in Vitro. We tested the ability of xylitol to reduce the
ASL salt concentration by applying a small volume (5 l) of
saline or xylitol to the apical surface. Twenty-four hours after the
saline was applied (138 mM ClϪ), non-CF epithelia reduced the
ASL ClϪ concentration to 45.3 Ϯ 1.3 mM (Fig. 3A). This value
Effect of apical xylitol on non-CF and CF ASL ClϪ concentration and
agrees with earlier measurements of ASL ClϪ concentration (9).
volume. Isosmotic xylitol or saline (5 l) was applied to the apical surface. Twenty-four hours later, ASL ClϪ concentration (A) and volume (B) were
When xylitol was applied instead of saline, the ASL ClϪ con-
determined. The asterisk indicates a difference between the saline and the
centration was even lower (34.2 Ϯ 4.3 mM).
xylitol solutions (P Ͻ 0.05; n ϭ 15–18) from three CF and three non-CF
In CF epithelia, the ClϪ concentration was 98 Ϯ 12 mM 24 h
11616 ͉ www.pnas.org
Effect of modifying ionic strength and xylitol concentration on killing
of E. coli by nasal lavage liquid. Nasal lavage liquid was diluted with increasingconcentrations of NaCl (bottom x axis) or xylitol (top x axis). SEMs are smallerthan the symbols.
fluid killed the bacteria. Although killing was inhibited as ionic
strength increased, killing was not affected by an increase in
xylitol concentration. We obtained similar results with P. aerugi-
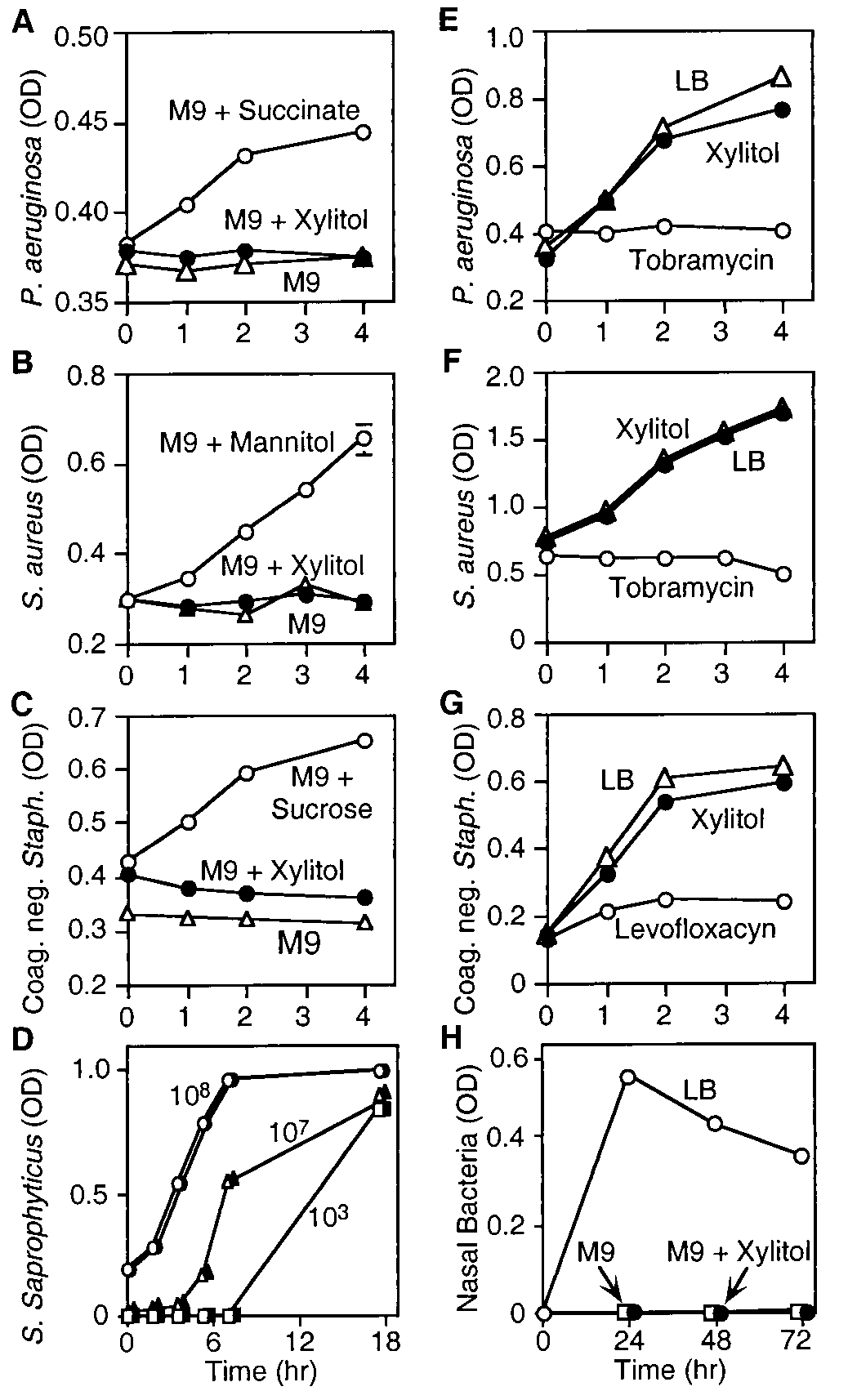
We asked whether xylitol would support the growth of the
predominant colonizers in CF lungs, P. aeruginosa and S. aureus.P. aeruginosa was placed in M9 medium, which lacks a carbon
source. Under these conditions, the bacteria showed no growth
(Fig. 5A). Adding the energy source succinate allowed bacterial
growth. In contrast, there was no growth of P. aeruginosa when
M9 medium was supplemented with xylitol. Likewise, xylitol
failed to support the growth of S. aureus or coagulase-negative
Staphylococcus (Fig. 5 B and C). Xylitol also failed to support the
growth of Staphylococcus saprophyticus, which ferments xylitol
(34) (Fig. 5D). To learn whether bacteria from the nasal surface
could use xylitol for growth, we obtained nasal swabs and
inoculated them into medium. The bacteria grew in LB medium,
whereas in M9 medium alone or M9 medium containing xylitol,
there was no growth (Fig. 5H). Although xylitol did not support
growth, it did not inhibit the growth of P. aeruginosa, S. aureus,
or coagulase-negative Staphylococcus in rich medium (Fig. 5
Effect of xylitol on growth of several bacteria. Growth of P. aerugi-E–G). As a positive control, we added a pharmaceutical antibi-
PHYSIOLOGY nosa (A), S. aureus (B), and coagulase-negative Staphylococcus (C) was mea-
otic to which the bacteria were sensitive.
sured as OD ‚, M9 medium alone. Xylitol (F) or succinate, mannitol, or sucrose
These results suggest that xylitol is relatively inert in terms of
(E) was added to M9 medium at 100 mM as indicated. (D) S. saprophyticus was
CF pathogens and bacteria on the nasal surface. It did not inhibit
grown in log phase in the presence (open symbols) and absence (closed
the effect of endogenous antibiotics, it did not serve as a ready
symbols) of xylitol for 18 h. Starting bacterial concentrations were 108 cfu
carbon source for growth, and it did not have antibiotic effects
(circles), 107 cfu (triangles), and 103 cfu (squares). P. aeruginosa (E), S. aureus
(F), and coagulase-negative Staphylococcus (G) were cultured in LB mediumalone (‚), LB medium with 100 mM xylitol (F), and LB medium containingtobramycin or levofloxacin (E). (H) Nasal swabs were collected and cultured
Xylitol Applied to Nasal Epithelia in Vivo Reduces the Number of
for 3 days in LB medium (E), in minimal M9 medium (ᮀ), or in M9 medium
Coagulase-Negative Staphylococcus. The ability of xylitol to lower
supplemented with 100 mM xylitol (F).
ASL ClϪ concentration in vitro and its relatively inert behavior
toward bacteria suggested the hypothesis that xylitol might lower
ASL salt concentration, thereby enhancing bacterial killing by
endogenous antimicrobial factors. However, as discussed above,
istered xylitol or a NaCl solution to both nostrils four times a day.
methods to accurately measure ASL salt concentration in vivo
After 4 days, the culture was repeated. After a 1-week recovery
remain problematic. Therefore, to test the concept, we examined
period, the study was repeated with the other treatment. The
the effect of xylitol administration on bacteria cultured from the
intervention (290 mM xylitol or 145 mM saline) for the first
nasal mucosa of normal subjects. Because pathogens such as P.
treatment was chosen at random. These agents were applied to
aeruginosa and S. aureus are uncommon on normal nasal mu-
both nostrils in 250 l with a preloaded syringe spray device.
cosa, we counted the number of coagulase-negative Staphylo-
Fig. 6 shows the median change in bacterial numbers after
coccus, an organism commonly found on the nasal mucosa
xylitol or saline administration. ANOVA for a crossover design
was applied to the change in bacterial count from pretreatment
We performed a randomized, double-blind, crossover study in
to posttreatment. The factors included in the ANOVA model
21 subjects. The number of coagulase-negative Staphylococcus
were treatment, sequence of treatment, and nostril side. Before
was determined by culture of nasal swabs. Subjects then admin-
the analysis a square root transformation (sign of change times
PNAS ͉ October 10, 2000 ͉ vol. 97 ͉ no. 21 ͉ 11617
airway infections develop, they may exist as biofilms that are
extremely resistant to antibiotics, including endogenous antimi-
crobial factors (35). Second, endogenous antimicrobial factors
are more important in the innate immune defense against small
numbers of bacteria; once infections develop, phagocytes and
the acquired immune system become more important. Third,
there is a significant inoculum effect, such that with large
numbers of bacteria the potency of endogenous antimicrobial
factors is reduced (7, 36). Fourth, in established infections, it
seems possible that bacteria might develop the ability to metab-
olize xylitol (37). However, we do not know whether the growth
of P. aeruginosa or other organisms is limited by the lack of
metabolic substrate. Finally, once established, infection and
inflammation alter the airway architecture, causing chronic
bronchiectasis, a difficult therapeutic challenge, even in patients
Effect of xylitol administration to nasal mucosa on coagulase-
negative Staphylococcus. Data are the decrease in colony-forming units of
coagulase-negative Staphylococcus after treatment with either saline or xy-
None of the subjects reported adverse effects of xylitol or
litol. Shown are median Ϯ one quartile. The asterisk indicates P ϭ 0.05.
saline. Although we have not rigorously tested for safety, we
predict that xylitol should be relatively nontoxic; it is present in
many foods, and it has been administered intravenously in large
square root change) was used to normalize the data. The analysis
doses to humans (38). In addition, other agents, including
showed that there was no significant effect of the sequence or the
hypertonic mannitol and hypertonic saline solutions, have been
nostril. Thus the comparison of xylitol vs. saline was evaluated
safely aerosolized to patients with bronchiectasis and CF to
from the data of both nostrils and both sequences. The average
improve cough and sputum clearance (39, 40).
reduction in the xylitol-treated nostrils was 597 Ϯ 242 colony-
Previous reports indicated that xylitol could reduce the growth
forming units (cfu) compared with 99 Ϯ 104 cfu for saline (P ϭ
of ␣-hemolytic Streptococci, including S. pneumoniae and S.
0.05). The median change was 500 (interquartile range of 1,152
mutans; however, it had little or no effect on Hemophilus
to 120) for xylitol and 89 (interquartile range of 540 to Ϫ53) for
influenzae or Moraxella catarrhalis (34). Moreover, we showed
saline (Fig. 6). Thus xylitol significantly reduced the number of
that xylitol did not have antimicrobial activity on its own against
coagulase-negative Staphylococcus on the nasal surface com-
coagulase-negative Staphylococcus or S. saprophyticus, yet when
administered to the surface of the nasal epithelium, it decreased
the number of coagulase-negative Staphylococcus. These data,
Discussion
plus the finding that xylitol lowered the ASL ClϪ concentration
By lowering the ASL ionic strength and enhancing the effec-
in vitro, suggest that the number of nasal bacteria decreased
tiveness of endogenous antimicrobials, xylitol administration to
because endogenous antimicrobial factors became more active.
the airway surface might be of value in preventing or delaying the
However, we have not measured a lower salt concentration in
onset of CF respiratory tract infections. Enhancing the activity
vivo (see above). Consequently, we cannot exclude the possibility
of endogenous ASL antibacterial factors could have significant
that xylitol reduced the number of bacteria by some other
advantages as a preventive strategy. These factors have broad-
mechanism. Although it is possible that mucociliary clearance
spectrum activity against Gram-positive and Gram-negative
was improved, we think this unlikely to be entirely responsible,
bacteria, including the organisms that are major CF pathogens
because the saline solution we administered as a control had no
(1–4). Because many of the factors kill very quickly (some within
significant effect. Nevertheless, it has been hypothesized that
minutes), conceivably even a transient enhancement of activity
mucociliary clearance is defective in CF airways because of a
might be of value. Importantly, most bacteria, even the major CF
reduced ASL volume (15). If this is the case, apical application
pathogens, do not show resistance to antibacterial peptides,
of xylitol might be of value, because our data show that it was
despite growth in the presence of subinhibitory concentrations.††
poorly permeable and increased ASL volume.
In striking contrast, when currently available pharmaceutical
Earlier reports have shown that xylitol used in chewing gum,
antibiotics are administered to prevent or treat CF infections,
in lozenges, or as syrup reduces the risk of caries and prevents
resistance rapidly emerges (6). P. aeruginosa is notorious in this
regard. Although in vitro acquired resistance to lysozyme has
acute otitis media (24, 25). In these applications, it is possible
been reported (32), it seems likely that resistance to the mixture
that xylitol may have enhanced mechanical clearance of bacteria
of endogenous factors will be uncommon, given the long period
without providing an energy source. However, the mechanisms
of coevolution of humans and bacteria. A recent report found
could be more complex. The mouth and oral pharynx contain
that aerosolized xylitol did not significantly reduce S. pneu-
endogenous antimicrobial factors (31). If xylitol administration
moniae nasal mucosal colonization in rats (33). This result is
lowers the salt concentration, the activity of those factors might
surprising because xylitol has been reported to have antimicro-
increase. In the case of acute otitis media, a small decrease in the
bial properties against this organism in vitro (34). Such results
total number of bacteria at the opening of the eustachian tube
highlight the need for human studies because the ASL antimi-
might decrease the frequency of middle ear seeding and infec-
crobial and electrolyte composition may vary significantly be-
tion. Our results, plus these considerations, suggest that using
xylitol to lower ASL salt concentrations could be of value for
Although xylitol might be of value in preventing airway
other applications, perhaps including prevention of ventilator-
infections, for several reasons we think it unlikely that enhancing
the activity of endogenous antimicrobials would be sufficient to
In conclusion, our data suggest that xylitol delivered to the
treat infections once they are established. First, when chronic
airway surface may enhance the innate antibacterial defense
system. These results suggest the hypothesis that xylitol or a
related osmolyte could prevent or slow the onset of bacterial
††Fujii, C. A., Boggs, A. F., Hurst, M. A. & Mosca, D. A. (1999) Pediatr. Pulmonol. Suppl. 19,
infection in CF. Further studies will be required to test this
11618 ͉ www.pnas.org
We thank Pary Weber, Tom Moninger, Norma Anderson, Xuihui Liu,
National Heart, Lung and Blood Institute; the Cystic Fibrosis Founda-
Sam McLennan, David Welsh, and Theresa Mayhew for excellent
tion; and the National Institutes of Diabetes and Digestive and Kidney
assistance. We thank Drs. Barbara Conway, Pradeep Singh, and Sue
Diseases) and the General Clinical Research Center (supported by
Travis for helpful discussions. We thank Drs. Leon Burmeister and
RR00059). This work was supported by the National Institutes of Health
Miriam Zimmerman for the statistical analysis. We appreciate the help
(HL42385, J.Z.), the Cystic Fibrosis Foundation, and the Howard
of the Iowa Statewide Organ Procurement Organization. We thank the
Hughes Medical Institute. J.Z. is supported by the Carver Charitable
University of Iowa In Vitro Cell Models Core (supported in part by the
Trust. M.J.W. is an Investigator of the Howard Hughes Medical Institute.
1. Lehrer, R. I. & Ganz, T. (1999) Curr. Opin. Immunol. 11, 23–27.
22. Bals, R., Wang, X., Wu, Z., Freeman, T., Bafna, V., Zasloff, M. & Wilson, J. M.
2. Huttner, K. M. & Bevins, C. L. (1999) Pediatr. Res. 45, 785–794.
(1998) J. Clin. Invest. 102, 874–880.
3. Bals, R., Weiner, D. J. & Wilson, J. M. (1999) J. Clin. Invest. 103, 303–307.
23. Holt, J. G., ed. (1984) Bergey’s Manual of Systemic Bacteriology (Lippincott,
4. Travis, S. M., Singh, P. K. & Welsh, M. J. (2000) Curr. Opin. Immunol., in press.
Philadelphia), Vol. 1, pp. 1016–1017.
5. Burns, J. L., Emerson, J., Stapp, J. R., Yim, D. L., Krzewinski, J., Louden, L.,
24. Edgar, W. M. (1998) Br. Dent. J. 184, 29–32.
Ramsey, B. W. & Clausen, C. R. (1998) Clin. Infect. Dis. 27, 158–163.
25. Uhari, M., Kontiokari, T. & Niemela¨, M. (1998) Pediatrics 102, 879–884.
6. Welsh, M. J., Tsui, L. C., Boat, T. F. & Beaudet, A. L. (1995) in The Metabolic
26. Yamaya, M., Finkbeiner, W. E., Chun, S. Y. & Widdicombe, J. H. (1992) Am. J.and Molecular Basis of Inherited Disease, eds. Scriver, C. R., Beaudet, A. L., Sly,
Physiol. 262, L713–L724.
W. S. & Valle, D. (McGraw-Hill, New York), pp. 3799–3876.
27. Zabner, J., Zeiher, B. G., Friedman, E. & Welsh, M. J. (1996) J. Virol. 70,
7. Smith, J. J., Travis, S. M., Greenberg, E. P. & Welsh, M. J. (1996) Cell 85,
8. Goldman, M. J., Anderson, G. M., Stolzenberg, E. D., Kari, U. P., Zasloff, M.
28. Cohen, J. (1988) Statistical Power Analysis for the Behavioral Sciences (Lawrence
& Wilson, J. M. (1997) Cell 88, 553–560.
9. Zabner, J., Smith, J. J., Karp, P. H., Widdicombe, J. H. & Welsh, M. J. (1998)
29. Citron, D. M., Edelstein, M. A. C., Garcia, L. S., Roberts, G. D., Thomson,
Mol. Cell 2, 397–403.
R. B. & Washington, J. A. (1994) in Bailey & Scott’s Diagnostic Microbiology,
10. Zhang, Y. & Engelhardt, J. F. (1999) Am. J. Physiol. 276, 469–476.
eds. Baron, E. J., Peterson, L. R. & Finegold, S. M. (Mosby, St. Louis), pp.
11. Baconnais, S., Tirouvanziam, R., Zahm, J.-M., de Bentzmann, S., Pe´ault, B.,
Balossier, G. & Puchelle, E. (1999) Am. J. Respir. Cell Mol. Biol. 20, 605–611.
30. Woods, G. L. & Washington, J. A. (1995) in Mandell, Douglas and Bennet’s
12. Joris, L., Dab, I. & Quinton, P. M. (1993) Am. Rev. Respir. Dis. 148, 1633–1637. Principles and Practice of Infectious Diseases, eds. Mandell, G. L., Bennett, J. E.
13. Knowles, M. R., Robinson, J. M., Wood, R. E., Pue, C. A., Mentz, W. M.,
& Dolin, R. (Churchill Livingstone, New York), Vol. 1, pp. 169–175.
Wager, G. C., Gatzy, J. T. & Boucher, R. C. (1997) J. Clin. Invest. 100,
31. Tenovuo, J., Luminkari, M. & Soukka, T. (1991) Proc. Finn. Dent. Soc. 87,
14. Hull, J., Skinner, W., Robertson, C. & Phelan, P. (1998) Am. J. Respir. Crit. Care
32. Fleming, A. (1929) Lancet 5501, 217–220. Med. 157, 10–14.
33. Kontiokari, T., Svanberg, M., Mattila, P., Leinonen, M. & Uhari, M. (1999)
15. Matsui, H., Grubb, B. R., Tarran, R., Randell, S. H., Gatzy, J. T., Davis, C. W. FEMS Microbiol. Lett. 178, 313–317.
& Boucher, R. C. (1998) Cell 95, 1005–1015.
34. Kontiokari, T., Uhari, M. & Koskela, M. (1995) Antimicrob. Agents Chemother.
16. Erjefa¨lt, I. & Persson, C. G. A. (1990) Clin. Exp. Allergy 20, 193–197. 39, 1820–1823.
17. Folkesson, H. G., Matthay, M. A., Frigeri, A. & Verkman, A. S. (1996) J. Clin.
35. Singh, P. K., Schaefer, A. L., Parsek, M. R., Moninger, T. O., Welsh, M. J. &
Invest. 97, 664–671.
Greenberg, E. P. (2000) Nature (London), in press.
18. Neville, M. C., Zhang, P. & Allen, J. C. (1995) in Handbook of MilkComposition, ed. Jensen, Robert G. (Academic, San Diego), pp. 577–675.
36. Thrupp, L. D. (1986) in Antibiotics in Laboratory Medicine, ed. Lorian, V.
19. Yamauchi, K., Tomita, M., Giehl, T. J. & Ellison, R. T. (1993) Infect. Immun.
(Williams & Wilkins, Baltimore), pp. 93–149. 61, 719–728.
37. Doten, R. C. & Mortlock, R. P. (1985) J. Bacteriol. 161, 529–533.
20. Travis, S. M., Conway, B. A., Zabner, J., Smith, J. J., Anderson, N. N., Singh,
38. Spitz, I. M., Rubenstein, A. H., Bersohn, I. & Bassler, K. H. (1970) Metabolism
P. K., Greenberg, E. P. & Welsh, M. J. (1999) Am. J. Respir. Cell Mol. Biol. 20, 19, 24–34.
39. Robinson, M., Regnis, J. A., Bailey, D. L., King, M., Bautovich, G. & Bye,
21. Singh, P. K., Jia, H. P., Wiles, K., Hesselberth, J., Liu, L., Conway, B. A.,
P. T. P. (1996) Am. J. Respir. Crit. Care Med. 153, 1503–1509.
Greenberg, E. P., Valore, E. V., Welsh, M. J., Ganz, T., et al. (1998) Proc. Natl.
40. Daviskas, E., Anderson, S. D., Eberl, S., Chan, H.-K. & Bautovich, G. (1999)
Acad. Sci. USA 95, 14961–14966. Am. J. Respir. Crit. Care Med. 159, 1843–1848. PHYSIOLOGY
PNAS ͉ October 10, 2000 ͉ vol. 97 ͉ no. 21 ͉ 11619
Available online at www.sciencedirect.comVeterinary Microbiology 133 (2009) 115–122Usage of antimicrobials and occurrence of antimicrobiala National Veterinary Institute, Technical University of Denmark, Hangøvej 2, Aarhus N DK-8200, Denmarkb University of Copenhagen, Faculty of Life Sciences, Department of Veterinary Pathobiology,Stigbøjlen 7, Frederiksberg C DK-1870, Denmarkc Natio
MAINE ASTHMA ACTION / MANAGEMENT PLAN Name: Date of Birth: Personal Best / Predicted Peak Flow: Symptoms: Action to Take: GREEN ZONE PEAK FLOW = ________ -- _______ You are doing great if : Continue to take your regular controller medicines every day (see blue box below) . You aren’t coughing, wheezing or having Controller medicine is not needed You
 Effect of apical xylitol on the rate of liquid absorption by non-CF and
CF epithelia. Sixty microliters of saline solution, xylitol solution, or indicatedmixtures of the two was applied to the apical solution. Four hours later thesolution was removed to measure the rate of liquid absorption. A shortincubation period was chosen to avoid secondary changes in the epitheliumdue to the large volume of apical liquid. Data are mean Ϯ SEM (n ϭ 15) fromthree different experiments. Some SEM bars are hidden by symbols.
Effect of apical xylitol on the rate of liquid absorption by non-CF and
CF epithelia. Sixty microliters of saline solution, xylitol solution, or indicatedmixtures of the two was applied to the apical solution. Four hours later thesolution was removed to measure the rate of liquid absorption. A shortincubation period was chosen to avoid secondary changes in the epitheliumdue to the large volume of apical liquid. Data are mean Ϯ SEM (n ϭ 15) fromthree different experiments. Some SEM bars are hidden by symbols.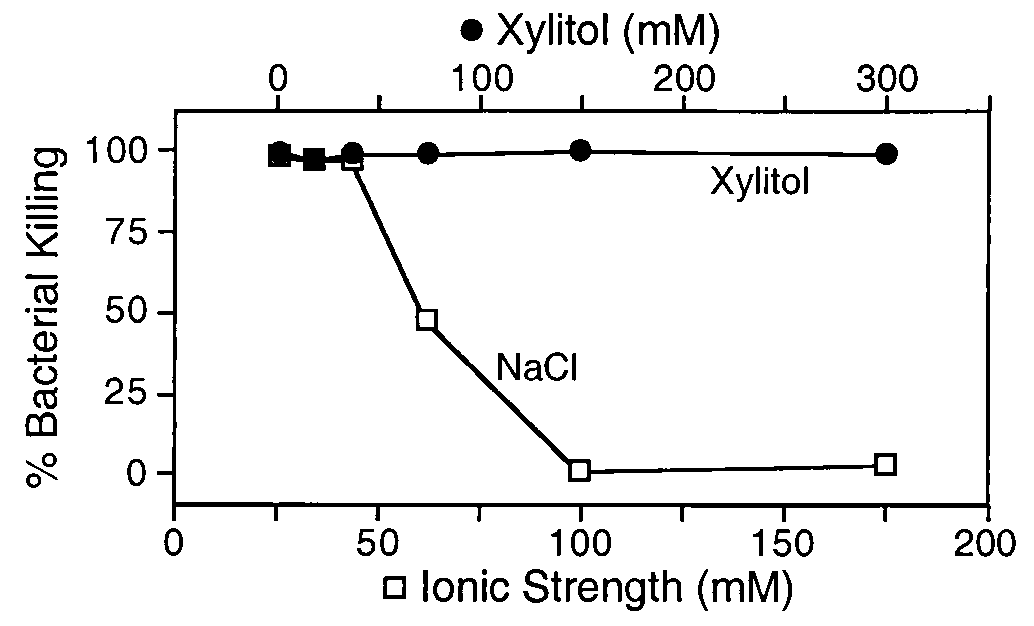
 Effect of modifying ionic strength and xylitol concentration on killing
of E. coli by nasal lavage liquid. Nasal lavage liquid was diluted with increasingconcentrations of NaCl (bottom x axis) or xylitol (top x axis). SEMs are smallerthan the symbols.
Effect of modifying ionic strength and xylitol concentration on killing
of E. coli by nasal lavage liquid. Nasal lavage liquid was diluted with increasingconcentrations of NaCl (bottom x axis) or xylitol (top x axis). SEMs are smallerthan the symbols.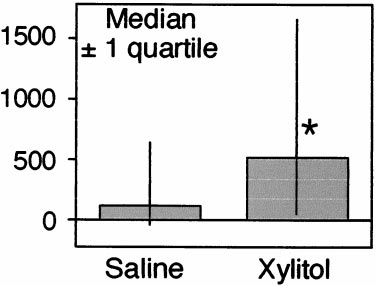 airway infections develop, they may exist as biofilms that are
extremely resistant to antibiotics, including endogenous antimi-
crobial factors (35). Second, endogenous antimicrobial factors
are more important in the innate immune defense against small
numbers of bacteria; once infections develop, phagocytes and
the acquired immune system become more important. Third,
there is a significant inoculum effect, such that with large
numbers of bacteria the potency of endogenous antimicrobial
factors is reduced (7, 36). Fourth, in established infections, it
seems possible that bacteria might develop the ability to metab-
olize xylitol (37). However, we do not know whether the growth
of P. aeruginosa or other organisms is limited by the lack of
metabolic substrate. Finally, once established, infection and
inflammation alter the airway architecture, causing chronic
bronchiectasis, a difficult therapeutic challenge, even in patients
Effect of xylitol administration to nasal mucosa on coagulase-
negative Staphylococcus. Data are the decrease in colony-forming units of
coagulase-negative Staphylococcus after treatment with either saline or xy-
None of the subjects reported adverse effects of xylitol or
litol. Shown are median Ϯ one quartile. The asterisk indicates P ϭ 0.05.
airway infections develop, they may exist as biofilms that are
extremely resistant to antibiotics, including endogenous antimi-
crobial factors (35). Second, endogenous antimicrobial factors
are more important in the innate immune defense against small
numbers of bacteria; once infections develop, phagocytes and
the acquired immune system become more important. Third,
there is a significant inoculum effect, such that with large
numbers of bacteria the potency of endogenous antimicrobial
factors is reduced (7, 36). Fourth, in established infections, it
seems possible that bacteria might develop the ability to metab-
olize xylitol (37). However, we do not know whether the growth
of P. aeruginosa or other organisms is limited by the lack of
metabolic substrate. Finally, once established, infection and
inflammation alter the airway architecture, causing chronic
bronchiectasis, a difficult therapeutic challenge, even in patients
Effect of xylitol administration to nasal mucosa on coagulase-
negative Staphylococcus. Data are the decrease in colony-forming units of
coagulase-negative Staphylococcus after treatment with either saline or xy-
None of the subjects reported adverse effects of xylitol or
litol. Shown are median Ϯ one quartile. The asterisk indicates P ϭ 0.05.